


- displaced frx of talar neck (no matter how slight) w/ subluxation or dislocation of posterior facet of sub-talar joint;
- subtalar joint subluxation is usually dorsal;
- ankle remains aligned;
- persistent slight displacement will result in malunion (usually in varus) which will produce an unacceptable result;
- despite posteromedial displacement of body with most type II injuries, posterior tibial neurovascular bundle is usually spared;
- however, it is manditory to monitor this neurovascular bundle;
- of greatest significance is high incidence (19% to 28%) of associated (usually medial) malleolar frx w/ this injury;
- complications include AVN in 30% and post-traumatic arthrosis in the majority of patients (over 2/3 patients);
- Exam:
- in addition to sig local soft tissue injuries, frxs of both remote & adjacent structures have been reported (64% in Hawkins series);
- Radiographic Evaluation:
- hawkins sign
- Treatment:
- in type II injuries caused by destruction of talocalcaneal ligament, it is difficult to perform closed reduction of dorsal & supination deformity;
- operate if there is > 3-5 mm of dorsal displacement & any rotational deformity;
- if closed reduction is possible then 8-12 weeks is necessary for healing (trabeculation across the fracture site);
- Closed Reduction:
- under adequate GEA, gentle traction is applied manually & foot is flexed plantarward to bring head frag into proper relaltion to body;
- any varus or valgus malalignment should be corrected as well;
- w/ foot held in equinus, lateral, and anteroposterior x-rays of talar neck should be taken to assess the adequacy of reduction;
- if an anatomical reduction has been achieved, the foot should be casted, still in equinus, in a short leg non wt bearing cast;
- this position should be held for 1 month, and then with subsequent casts the foot can be brought out of equinus as long as reduction is maintained;
- non wt bearing cast immobilization is usually required for 3 months to achieve bony union;
- varus angulation may occur w/ non operative treatment;
- occurs due to medial comminution;
- the main effect of this is to eliminate subtalar motion;
- Open Reduction:
- if reduction is not maintained, operative treatment is indicated;
- consider longitudinal anteromedial incision over talar neck just medial to anterior tibial tendon;
- this allows direct acces to the fracture site;
- an anterolateral approach may decrease chance of further damage to blood supply of talus and provides adequate exposure of the fracture;
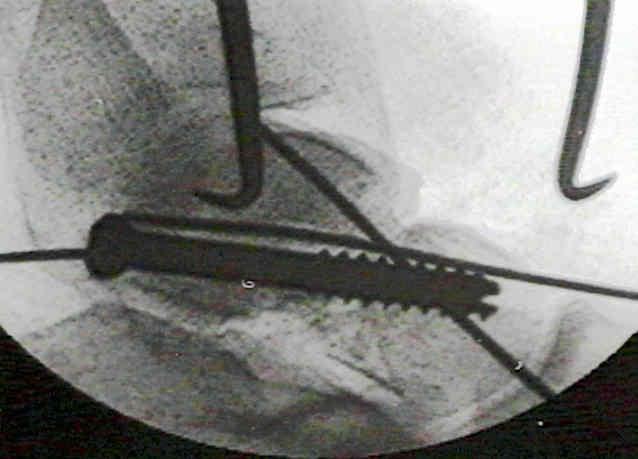
- following K wire fixation (and ORIF such as a lag screw) a non wt bearing cast is applied for 8-12 weeks, or until frx is healed;
- rigid internal fixation may be achieved using AO cancellous screw once fracture is anatomically reduced;
- when there is comminution of the medial neck, screw compression can produce a varus deformity;
- placement of the screw from posterolaterally to anteromemdially can help avoid this problem;
- Complications:
- avascular necrosis and/or degenerative arthitis can be expected in over 1/2 cases
-------------------------------------------------
A new look at the hawkins classification for talar neck fractures: which features of injury and treatment are predictive of osteonecrosis?