

- End to Side Technique - Large Vessel Repair Donald Serafin M.D.
- End to End - Large Vessel Repair Duke University Medical Center
- Vein Grafting
- PreOp Preparation:
- pharmocological agents;
- vessel dilators;
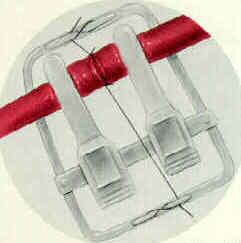
- approximator clamps;
- clamp contains two atraumatic clamps attached to a retangular frame;
- monofilament nylon;
- sizes range from 8-0 to 11-0 w/ 75 micrometer needle;
- 10-0 suture is used for digital vessels;
- bipolar cautery;
- Vessel Exposure & Preparation:
- resect vascular wall until the cut ends appear normal;
- repairing rather than resecting injured vessels to avoid using vein grafts will usually fail due to vessel thrombosis;
- mobilize both ends of vessel to obtain adequate length for anastomosis;
- mobilize vessel ends to allow approximation w/ minimal tension;
- this usually requires 2 to 3 cm;
- remove the loose conective tissue surrounding the vessel;
- colored plastic sheet is placed beneath vessel to make it easier to see;
- cauterize tethering side branches w/ bipolar electrocautery;
- small branches may be electrocoagulated 2-3 mm from parent vessel;
- irrigate operative field w/ heparinized Ringer's lactate solution;
- blood is cleared from vessel ends by jet of saline;
- continue to irrigate the field intermittently with heparinized Ringer's lactate;
- use a 25 to 30 gauge blunt tipped needle;
- vessel dilitation
- first performed w/ pharmologic agents (1% lidocaine);
- if this is not optimal, dilitation is performed mechanically, dilitating the ends 1.5 times normal diameter;
- there is some evidence that this may injure the intima;
- approximator clamps;
- clamp contains two atraumatic clamps attached to a retangular frame;
- vessel ends are placed within the jaws of the clamp approximator and are positioned to permit clamp to be flipped 180 deg w/o tension;
- damaged vascular clamps which exert greater than 30 gms/ sq mm may cause endothelial damage and subsequent thrombosis;
- vessels should be clamped w/ the minimal effective pressure;
- initially slide the clips as far apart as possible;
- once vessel ends have been placed in clips, use forceps to gently slide the clips together, which will approximate the vessels;
- adventia is removed from vessel wall;
- pull adventia down over vessel end, cut it, & let it retract;
- adventia may also be removed by careful circumferential trimming;
- adventia should be stripped from the vessel ends approximately 2 mm, to prevent accidental incorporation of adventia in suture;
- remove sufficient adventia from the vessel ends to expose all layers of the vessel wall;
- anticoagulation:
- before the vascular anastomosis give systemic heparin;
- Suture Technique:


- initial suture insertion: (inside to out)
- use double armed suture to insert needle from "inside to out" on both sides of the anastomosis;
- this ensures that the intimal edges will be everted;
- use interrupted sutures to prevent vascular constriction, and place each suture thru the full thickness of the vessel wall;
- avoid suturing both walls together;
- this is best managed by prevention;
- this complication can be difficult to identify once the sutures have been placed;
- place first two stay sutures approximately 120 deg apart on vessels circumference;
- leave the ends of these sutures long for use as traction sutures;
- by placing the two stay sutures 120 deg apart, the posterior (back wall) will fall away, making it less likely to capture both walls;
- rotate clamp approximators to expose posterior vessel wall & place
stitch 120 deg from initial two stitches;
- first stay suture applied with the tip of forceps in lumen to protect back wall from needle and to provide counter pressure;
- 2nd stay suture placed at 1/3 of vessel circumference away from 1st;
- this allows the back wall to drop away, protecting it from the needle;
- place more stitches in remaining spaces to complete anastomosis;
- arteries 1 mm in diameter usually require 5 to 8 stitches, and veins require 7 to 10 stitches;
- vessels may be gently dilated by insertion of tips of jewler's forceps;
- walls of vessels may be grasped, but avoid rough manipulation of intima;
- to overcome vascular spasm, apply topical lidocaine or papaverine;
- completion of anastomosis:
- after anastomosis is complete, first remove the distal clamp;
- look for back filling in the vessel across the suture line, a small amount of oozing is normal;
- cut the stay sutures and remove the clamp which is upstream;
- if excessive bleeding is present, place additional stiches in the areas of leakage, remove clamps again, and deflate the tourniquet;
- assess the patency of anastomosis by occluding a segment of vessel distal to the anastomosis;
- completion of anatomosis:
- in the report by Chen, et al, the authors compared continuous vs interrupted suture technique;
- total thrombosis rate was 8%, but no significant patency difference was noted between the CST and the interrupted suture technique in any vessel category.
- ref: Comparison of continuous and interrupted suture techniques in microvascular anastomosis.
- Technique of anastomosis of larger vessels
- considerations:
- prosthetic grafts
- vascular shunts
- initial preparation:
- prepare wide operative field & prepare opposite extremity for possible reversed saphenous be bypass graft;
- debridement:
- dilute heparin solution is flushed down the distal arterial bed;
- embolectomy catheters are then used to remove thrombus;
- intima is examined, extending arteriotomy as necessary;
- obtain control of artery distal to presumed site of injury to minimize loss of blood by back bleeding;
- inspect & palpate the site of injury to determine need for repair;
- proximal and distal controls should be obtained at least 2 to 3 cm from site of injury so that intima can be examined;
- in both penetrating and blunt trauma, the intima may be damaged beyond the obvious site of injury;
- damaged intima requires resection;
- remove proximal clot by flushing & distal clot by milking vessel, squeezing the distal limb, or passing a Fogarty balloon catheter;
- excess advential tissue is excised from outer surface of vessel so that it will not be dragged into the anastomosis;
- observe intimal as it is flushed with heparinized saline to see if there is evdience of an intimal flap;
- before anastomosis, determine need for graft replacement by estimating amount of difficulty in approximating the severed ends;
- in general, 1-2 cm of artery may be resected w/o graft replacement;
- arterial anastomosis should not be performed under tension;
- repair injured artery w/ interrupted or continuous fine monofilament sutures;
- smaller arteries may be constricted using continuous suture techniques;
- in children, interrupted suture repair is preferred to ensure circumferential growth;
- prior to completion of repair, arteries are forebled and backbled;
- closure consists of a interrupted suture, placed close together, run down the proximal aspect of the artery;
- using a double armed needle, both sutures are passed inside to out inorder to ensure intimal eversion;
- sutures pass thru all layers, particular care being taken to include intima;
- suture bites taken 1 mm apart and 1 mm from edges, unless vessels are large, thick walled or diseased;
- arteries need to be black bled and flushed, using heparin- dextran solution, followed by flushing with a dextran solution;
- completion arteriogram is performed to assess quality of vascular reconstruction for intimal defects, suture line problems, and the adequacy of the distal runoff;
- Post Operative Management:
- see pharmocological agents used in vascular surgery;
- proper hydration of pt, warm environment, adequate analgesia, avoidance of hypotension, and a ban on smoking
References for Arterial Trauma
The effect of microvascular anastomosis configuration on initial platelet deposition.
The strength of microvascular anastomoses--an experimental evaluation in rats.
The Use of Arteriovenous Anastomosis for Replantation of the Distal Phalanx of the Fingers.
Early microsurgical reconstruction of complex trauma of the extremities.
Spatulated versus end-to-end anastomosis for small vessel injury.
Comparison of continuous and interrupted suture techniques in microvascular end-to-side anastomosis.
Evaluation of clinical microvascular anastomoses--reasons for failure.
Management of the contused arterial segment.