

- See: Anatomy of Carpal Tunnel
- Incision: 

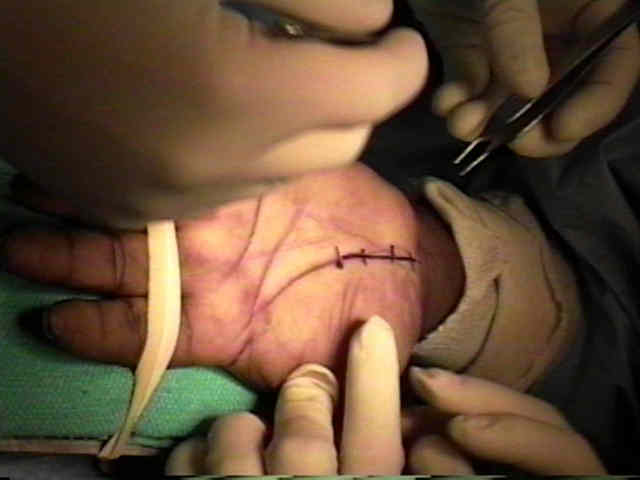

- incision is made parallel and just ulnar to the thenar crease overlying the TLC;
- incision is generally placed 2-3 mm medial to thenar crease, in line with the long axis of the ring finger;
- proximally, there is usually no need to cross the most distal volar wrist crease (since this may be associated w/ pillar pain);
- the exception might be acute carpal tunnel syndrome, in which the longer incision may be required;
- distally, the incision extends to a point just shy of the level of the superficial palmar arch;
- horizontal line that is in line w/ distal border of outstretched thumb
- once down to the subcutaneous tissue, consider dissecting the subQ tissue off of the palmar aponeurosis both radially and ulnarly inorder to achieve better exposure;
- a more radially placed incision, risks injury to the palmar cutaneous branch (as well as the recurrent motor branch);
- a more ulnarly placed incision risks injury to contents of Guyon's Canal;
- Proximal Skin Extension:
- this incision allows proximal isolation of nerve, & allows visualization of abnormal muscles or proliferative flexor sheath synovium;
- it is better to avoid incision directly on volar crease because it serves as natural hinge in skin during flexion of thumb;
- it should be noted that incisions that cross the wrist crease at right angles may result in a hyper-trophic and painful scar, as well as a wrist flexion contracture;
- optional extension of incision may be made into wrist in S shaped curve, but this is seldom necessary;
- if incision needs to be extended proximally, it is turned toward ulnar side to avoid palmar cutaneous branch;
- two incision technique:
- involves making a proximal transverse incision at the wrist, which allows proximal entry into the carpal tunnel (and protection of the median nerve), and allows easier release of the proximal palmar fascia;
- avoids the need for the standard carpal tunnel incision across the wrist;
- flex the patient's wrist and choose the wrist crease that best separates the mobile forearm skin from the palmar skin;
- if it is difficult to choose between the proximal and distsal creases, choose the proximal crease;
- the transverse incision should generally be made proximal to the pisiform since this helps form the roof of the carpal tunnel;
- make a 2-3 cm transverse incision between the FRC and FCU tendons;
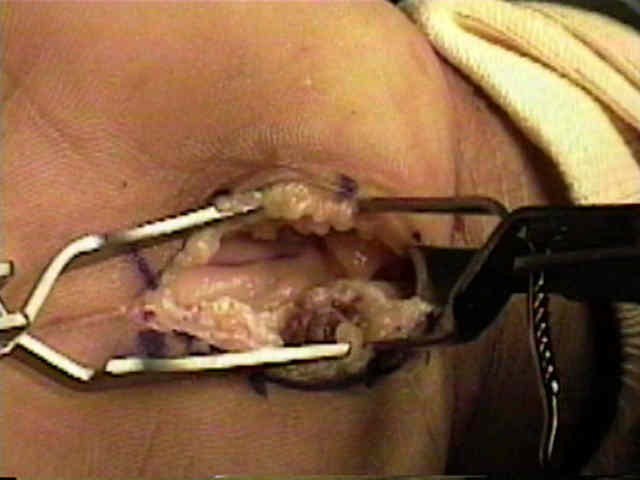
- a distsally based flap of superficial fascia is created and is elevated w/ a small clamp;
- immediately underneath this fascia lies the median nerve;
- use a blunt elevator to sweep the synovium off of the deep surface of the fascia;
- probing the undersurface of the TCL should give a washer-board sensation;
- if washer-board sensation is not present then the probe is either in Guyon's Canal or is superficial to the TLC;
- references:
- An open twin incision technique of carpal tunnel decompression with reduced incidence of scar tenderness.
- [Double incision for operation of carpal tunnel syndrome--14 years experience.]
- Hazards:
- above wrist, it is important to distinguish median nerve from flexor tendons;
- nerve at this level may resemble a tendon because it is flattened rather than round, but in living body nerve is normally whiter and has fine vessels on its surface;
- palmar cutaneous branch:
- palmar cutaneous branch of median nerve arises from its main trunk, about 4 cm proximal to the wrist crease (lies just deep to the superficial veins).
- keep the incision away from palmar cutaneous branch of median nerve since injury to this branch can result in intractable neuroma tenderness;
- to avoid palmar cutaneous branch, incision needs to be on ulnar border of palmaris longus);
- superficial palmar arch:
- at distal palm, superficial palmar arch crosses volar to nerve & is protected;
- superficial transverse arch, which lies at distal end of the carpal canal, must not be looked for and not injured
Flexor carpi radialis approach for carpal tunnel release.
Distribution of nerve fibers in the standard incision for carpal tunnel decompression.
[Double incision for operation of carpal tunnel syndrome--14 years experience.]
Local symptoms after open carpal tunnel release. A randomized prospective trial of two incisions.
Double incision open technique for carpal tunnel release: An alternative to endoscopic release.