

 - Anatomy:
- Anatomy:
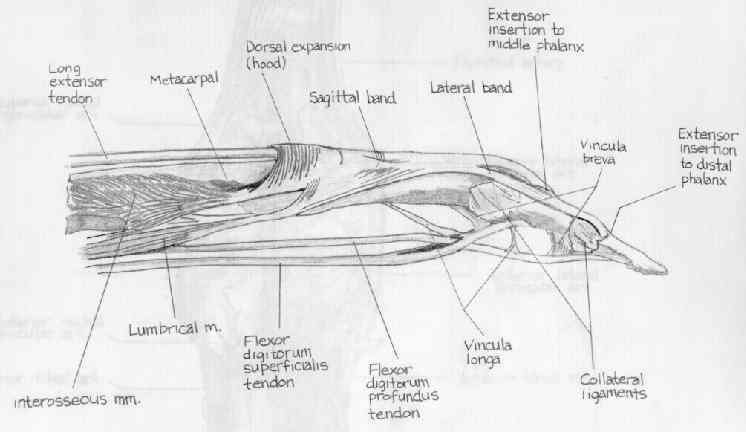
- on volar aspect of finger, FDP passes through FDS to insert on distal phalanx;
- both long flexor tendons are tightly enclosed in common tendon sheath which corresponds to zone II;
- anatomical proximity explains the development of adhesions between FDS & FDP tendons & digital
fibrous sheaths following injury;
- excursion of tendons
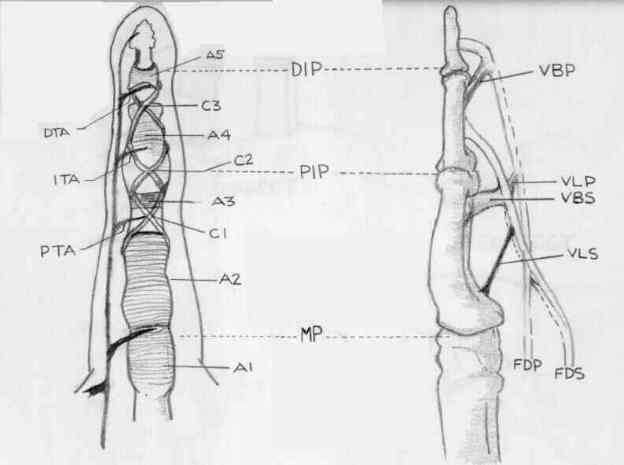
- tendon sheath anatomy
- Partial Laceration of Flexor Tendons
- Primary Tendon Repair:
- tendon injuries are usually repair primarily, esp in clean wounds;
- surgical approach and statedgy are dependent on location of tear:
- FDS Laceration
- FDP Laceration (FDP avulsion)
- Zone I Injuries
- Zone II injuries
- Zone III injuries
- Zone IV and Zone V
- Tendon Repair Technique:
- core suture techniques;
- optimizing tension in flexor tendon repair:
- Primary Flexor Tendon Grafting
- Staged Flexor Tendon Repair:
- optimizing tension in flexor tendon repair
- prosthetic Grafts
- pulley reconstruction
- complications:
- delayed primary repair is complicated by enlargement of proximal tendon end, which contracts into palm and thus cannot be
passed back through narrow digital sheath;
- adhesions will also restrict tendon from entering the tendon sheath;
- if these conditions are encountered then consider a tendon graft;
- Pulley Reconstruction:
- Tendon Sheath Anatomy
- Complications:
- tendon rupture
- adhesion formation: (see: flexor tenolysis)
- adhesions form if part is immobilized because the wound in sheath and wound in the tendon grow together;
- if part is kept mobile, they heal separately, and function is more likely to be restored;
- collagen tensile strength across the repair is not sufficient to permit active loading for 4-5 weeks
- on exam, patient will demonstrate loss of active flexion, but relative maintenance of active extension and maintenance of
passive flexion;
- severe adhesion formation is managed with tenolysis
- ref: Effects of Nonsteroidal Anti-Inflammatory Drugs on Flexor Tendon Adhesion
- flexion contracture:
- may occur in up to 20%;
- distinguish between true flexion contracture (loss of both active and passive ROM) and flexor tendon adhesions (loss of active
ROM only);
- occurs as a result of holding finger in the flexed position;
- swan neck deformity:
- especially likely to happen, in pts w/ hyperextensible PIP joint;
- can occur after primary repair of FDP or free tendon grafting;
- may result from complete excision of FDS;
- see: swan neck deformity following FDS harvest;
- when FDS is exised at its insertion, the vinculum is also excised, which damages the checkrein of PIP allowing to fall into
hyperextension;
- as extensor apparatus becomes lengthened from PIP hyperextension, the terminal phalanx will sag into flexion;
- lateral bands displace dorsally;
- to prevent swan neck deformities:
- avoid excision of FDS farther distally than neck of middle phalanx or just proximal to the vinculum
- references:
- Treatment of unfavourable results of flexor tendon surgery: Ruptured repairs, tethered repairs and pulley incompetence.
Angiogenesis in healing autogenous flexor-tendon grafts.
Autogenous flexor-tendon grafts. A biomechanical and morphological study in dogs.
Work of flexion after flexor tendon repair according to the placement of sutures.