


- Discussion:
- results from a defect is somatic mutation in the gene coding for alpha subunit of Gs, the G protein that stimulates cAMP formation;
- overproduction of cAMP, causes overexpression of c-fos, which regulates proliferation and differentiation of osteoblasts and osteoclasts;
- results in lesions of bone which results in a haphazard mixture of immature fibrous tissue & small fragments of immature trabecular bone;
- angular deformities may result from defective mineralization of immature of immature dysplastic bone;
- affected bone becomes widened and adjacent cortical bone becomes thin;
- occurs typically in adolescence;
- prevalence of malignant transformation (chondrosarcoma or osteosarcoma) is about 0.4 %;
- sites of involvement:
- rib is involved most often but any bone can be involved;
- also seen in proximal femur, proximal tibia, mandible;
- pathologic frx:
- bone becomes deformed by multiple stress frx which may eventually lead to pathologic frx;
- painful stress frxs are esp common in femoral neck;
- although dysplastic bone heals at nl rate after frx, resulting callus is also dysplastic, and the disease persists;
- prognosis:
- progression of the disease is often erratic;
- monostotic lesions: have good prognosis;
- polyostotic lesions:
- tend to remain more active or aggressive;
- are known to occassionally undergo malignant transformation to osteosarcoma or fibrosarcoma.
- Associated Conditions:
- Albrights Syndrome (McCune-Albright syndrome)
- precocious puberty and cafe au lait pigmentation in females;
- child w/ monostotic fibrous dysplasia usually has no symptoms;
- polyostotic dz, which usually presents earlier, may be unilateral or widespread, affecting long bones, hands, feet, & pelvis;
- prevalence of malignant transformation (chondrosarcoma or osteosarcoma) is about 4 %;
- references:
- Some aspects of polyostotic fibrous dysplasia: possible hypothesis to account for the associated endocrinological changes.
- Dedifferentiated chondrosarcoma in Albright syndrome. A case report and review of the literature.
- Intravenous pamidronate treatment of polyostotic fibrous dysplasia associated with the McCune Albright syndrome.




- Clinical Presentation:
- lesions may occur in one bone (monostotic) or in many (polyostotic),
- occasionally, a child may present w/ pathologic frx or angular deformity;
- polyostotic fibrous dysplasia:
- children present around age 10;
- findings include pain, pathologic frx, limp, or limb deformity;
- in general osseous abnormalities present before age 20 yrs;
- upper extremity:
- on occassion, non wt bearing joints may be severely involved;
- Radiographs:
- appearance of lesions is variable but most often will show:
- intramedullary diaphyseal lesion that blends w/ thinned, bulged cortex;
- hazy or ground glass lesion which may occur w/ angular deformity;
- angular deformity in bone is often present at the level of lesion;
- active lesion may progress in size and deformity;
- cystic type of lesion:
- radiolucent w/ a reactive rim, no trabeculae, & normal cortical thickness;
- pagetoid type of lesion:
- trabecular pattern which is more dense than normal bone;
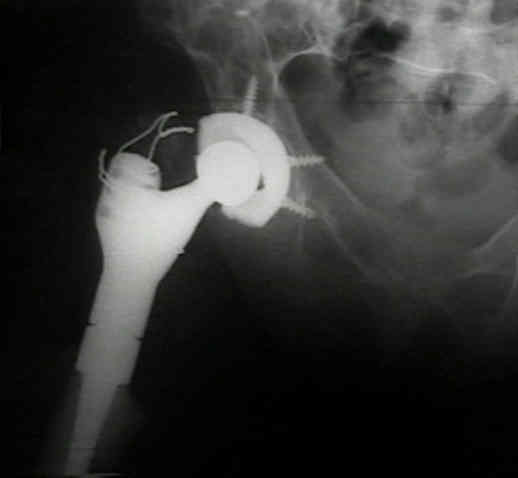
- shepherd's crook deformity:
- extensive involvement of proximal femur results in a characteristic varus deformity which resembles a shepherd's crook;
- Bone Scans:
- reveals intense radioistope uptake that reflects the extent of tumor seen on x-ray, esp when the lesion is active;
- a decrease in bone scan activity implies that dz has become inactive;
- CT scan: may help evaluate extent of bone involvement;
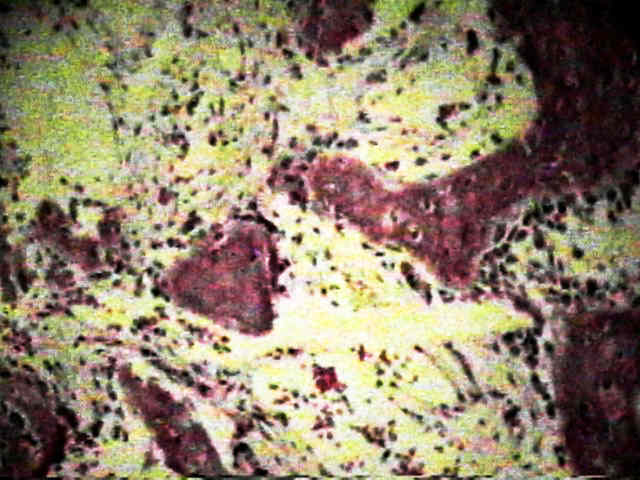
- Histology:
- there is an irregular collection of small pieces of immature woven trabeculae sorrounded by abundant
fibroblastic proliferation of matrix of fibrous tissue and immature woven trabeculae;
- appearance has been likened to that of alphabet soup, w/ trabeculae resembling Cs, Os, & Us;
- trabeculae:
- appear immature:
- are not lined with osteoblasts (as in ossifying fibroma);
- do not contain cement lines;
- do not remodel according to stress;
- fibrous stroma is disorganize & replaces normal marrow;
- diff dx:
- osteoblastoma, osteosarcoma, ossifying fibroma, hyperparathyroidism, and Pagets Disease
- Treatment:
- medical treatment: consider biphophonate treatment (fosamax);
- in the study by Lane JM, et al (2001), the combination bisphosphonate therapy diminished pain, prevented fractures, lowered
N-telopeptide values, and led to partial resolution of fibrous dysplasia lesions;
- ref: Bisphosphonate therapy in fibrous dysplasia.
- preop considerations:
- note that adults may experience intra-operative hypoxemia and shunting during surgery (? due to AV shunting), and that these
patients may benefit from intra-operative Swan Ganz monitoring;
- goal of management is prevention of the deformity and fracture;
- treatment of fibrous dysplasia involves strengthening & straightening involved bone;
- resection & curretage is not indicated, since dysplastic bone usually recurs;
- recurrence rate with simple curettage and bone grafting, esp in pediatric age group is high;
- large lesions with an angular deformity are best straightened and grafted with cortical bone;
- cortical bone is less likely to be resorbed than cancellous bone and is more likely to provide permanent structural support;
- this is best acomplished using cortical bone autografts (taken from fibula), which minimally remodels after incorporation.
- grafting w/ cortical bone is particularly appropriate for managing lesions in high stress areas such as the femoral neck;
- alternative treatment methods are reconstruction with cortical bone allografts or fixation with an intramedullary rod;
- radiation treatment has not been shown to be effective in erradicating the disease and may infact lead to malignant transformation;
- lower extremity:
- progressive coxa vara deformity is common which can eventually lead to the Sheppard's crook deformity;
- vast majority of patients with polyostotic lesions will have involvement of the proximal femur and in most of these patients,
there will be more frequent and more severe involvement of the calcar which means that it will be unable to support
internal fixation;
- indications for surgery include progressive deformity, persistent pain, and failure of conservative treatment;
- pending pathologic frx in heralded by 2.5 cm (or greater) lytic lesion involving the proximal femur;
- valgus osteotomy and internal fixation: this is best performed early in the disease;
- medial displacement osteotomy: involvement of the calcar or poor bone quality
- cortical window is used both for removal of fibrous tumor tissue and for bone grafting;
- upper extremity:
- pathologic frx of upper extremity can be treated closed in contrast to lower extremity pathologic fractures which should
be fixed internally;
- Case Example:




Fibrous dysplasia of the femoral neck. Treatment by cortical bone-grafting.
Bone-Grafting in Polyostotic Fibrous Dysplasia
Fibrous dysplasia. An analysis of options for treatment.
Critical review of infantile fibrous dysplasia: surgical treatment.
The histopathology of fibrodysplasia ossificans progressiva. An endochondral process.
Treatment of fibrous dysplasia involving the proximal femur.
Fibrous Dysplasia in the Spine: Prevalence of Lesions and Association with Scoliosis.
Fibrous dysplasia. Pathophysiology, evaluation, and treatment.