

 - See:
- See:
- Adult Condylar Fractures
- Distal Humeral Nonunion
- Humeral Fractures
- Non Operative Treatment: (cast bracing);
- some orthopaedists do not feel that Holestein Lewis Frx are amenable to cast bracing;
- some of these fractures are amenable to cast bracing and often elbow stiffness (most feared complication)
is not a problem;
- Sarmiento, et al (1990), 85 extra-articular comminuted distal 1/3 humeral frx in adults were followed during 5 year period;
- all patients were managed with prefabricated braces;
- 15% were open fractures and 18% had initial peripheral nerve injury;
- braces were kept in place for an average of 10 weeks;
- there was 96% union, with no infections
- all nerve injuries or resolved or were improving at the latest examination;
- at union there was varus deformity averaging 9 degrees in 81% of patients, but loss of range of movement was minimal and
functional results were good;
- references:
- Functional bracing for comminuted extra-articular fractures of the distal third of the humerus
- Functional treatment of the distal third humeral shaft fractures.
- Operative Treatment:
- plate fixation of humerus;
- anterolateral approach:
- Modified anterolateral approach for internal fixation of Holstein-Lewis humeral shaft fractures.
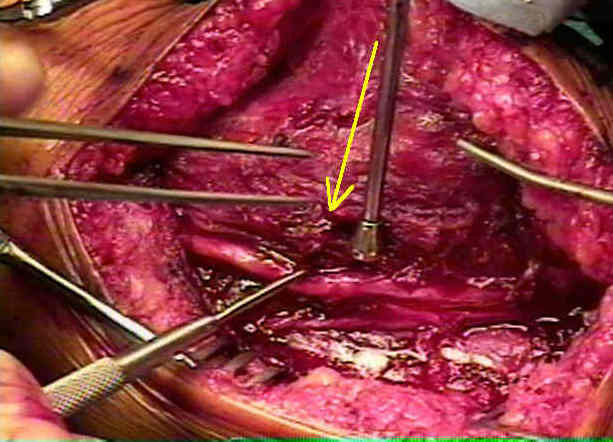
- posterior approach to the humerus;
- humerus is flat posteriorly and it is easier to apply the broad plate to that surface & plate can also reach further distally w/o
comprimising flexion;
- fracture may be stabilized w/ a 4.5 mm DC plates;
 - Complications:
- Complications:
- radial nerve palsy associated w/ humeral shaft frx:
- upto 18% of humeral shaft frx have an associated radial nerve palsy, but may occur more commonly
in distal third fractures;
- radial nerve is commonly at risk if the fracture is at the junction of mid and distal thirds of the
humeral shaft and particularly if frx is associatted with lateral displacement of distal fragment;
- at this point the radial nerve emerges from the spiral groove and is tethered as it pierces the
intermuscular septum;
- it cannot yeild to the lateral displacement of the distal fragment, and is therefore frequently damaged;
- most nerve injuries represent a neuropraxia or axonotmensis;
- 90% will resolve in three to four months
Fractures of the Humerus with Radial Nerve Paralysis.
A Biomechanical Analysis of Prophylactic Fixation for Pathological Fractures of the Distal Third of the Humerus.
Intraarticular fractures of the distal humerus in the adult.
Intraarticular fractures of the distal humerus. Surgical treatment and results.
Mechanical failures of internal fixation in T and Y fractures of the distal humerus.
A contemporary approach to the management of complex fractures of the distal humerus and their sequelae.
Extra-articular distal-third diaphyseal fractures of the humerus. A comparison of functional bracing and plate fixation.
The Holstein-Lewis humeral shaft fracture: aspects of radial nerve injury, primary treatment, and outcome
Operative treatment of distal humeral fractures in the elderly.