

- most often used for anterior shoulder reconstructions


- Positioning: 
- beach chair w/ full access to posterior aspect of shoulder;
- holding shoulder in flexion, will relax shoulder & facilitate exposure;
- consider the Mconnel Shoulder Positioner;
- references:
- The prevention of injuries of the brachial plexus secondary to malposition of the patient during surgery.
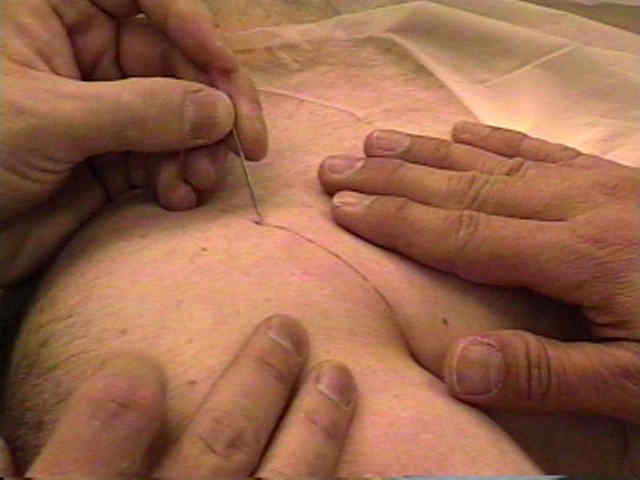 - Incision:
- Incision:
- incision is marked w/ needle in major axillary skin fold w/ the arm adducted;
- depending on patient's size, the incision will pass up toward coracoid process;
- skin incision begins in the axilla and is centered over pectoralis major tendon;




- if a larger incision is required, extend it toward coracoid;
- the skin must be mobilized by undermining a full thickness layer of subQ tissue overlying the fascia;
- identify the the coracoid which serves as a landmark for brachial plexus (lying medially) and the cephalic vein
(lying inferiorly);

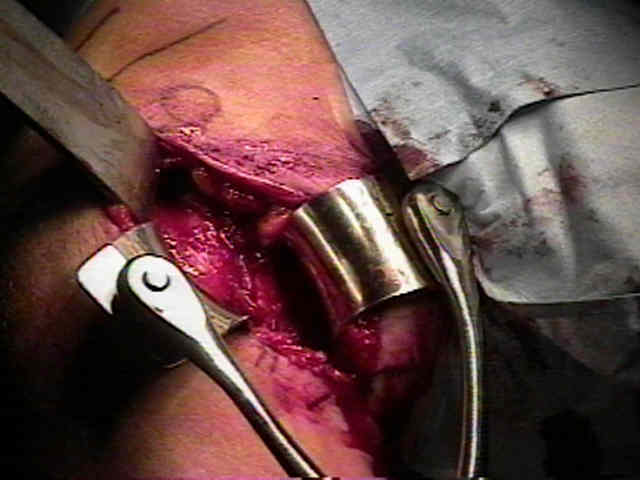
- Delto-Pectoral Interval:
- skin and the subcutaneous tissue are undermined up to the level of the coracoid process;
- cephalic vein: marks the location of the deltopectoral interval;
- cephalic vein proceeds superiorly over the coracoid on its way to the subclavian vein;
- if the cephalic vein is not visible, look for a fat strip which may overlie the vein;
- in most cases, the vein is retracted laterally (along w/ the deltoid) because it is usually more adherent to the
deltoid (preserving the deltoid's venous drainage) and because deltoid branch of thoracoacromial artery
lies parallel and lateral to cephalic vein and supplies blood to deltoid;
- the easiest way to develop the deltopectoral interval is to dissect downward just medial to the cephalic vein;
- avoid the temptation of defining the interval between the superficial muscle fibers;
- often the true interval lies more lateral than is expected;
- deltopectoral interval may be developed all the way up to the clavicle, but in most cases there is no need to detach deltoid from clavicle;
- in upper 1/3 of deltopectoral interval, branch of thoracoacromial artery & lateral pectoral nerve this bundle is cauterized and transected;
- subdeltoid and subpectoral spaces:
- these spaces need to be developed by blunt dissection down to their muscular insertions;
- at times the medial edge of the deltoid is covered by clavi-pectoral fascia, in which case, it should be sharply transected, to allow entry tosub-deltoid space;
- in upper 1/3 of deltopectoral interval, branch of thoracoacromial artery & lateral pectoral nerve this bundle is cauterized and transected;
- at this point, a self retaining retraction can be insert beneath each muscle;
- extensile measures:
- generally the deltopectoral groove is opened distally until the insertion of the pectoralis is reached;
- deltoid muscle:
- anterior 1/3 of the deltoid insertion may be elevated for further posterolateral exposure;
- on occassion, a small portion of the deltoid can be dissected off the clavicle, allowing flap of muscle to be reflected more laterally;
- pectoralis muscle:
- incise the cephalad 1-3 cm of the pectoralis major tendon inorder to achieve better exposure of the inferior portion of the subscapularis tendon
(and better protection of the axillary nerve);
- detaching the upper 1-2 cm of the pectoralis will also better visualize the inferior capsule & axillary nerve, which passes just inferior to the capsule;
- if the shoulder has a severe internal rotation contracture, consider release of the entire tendon;
- note that the remaining internal rotators are intact (latissimus, teres major, and subscapularis);
- use the long head of the biceps to help locate the insertion of the pectoralis (placing arm in abduction and internal rotation may also help with exposure);
- long head of the biceps emerges from the bicipital groove at a point just above the insertion of the pectoralis, and can be injured when the
pectoralis insertion is partially incised;
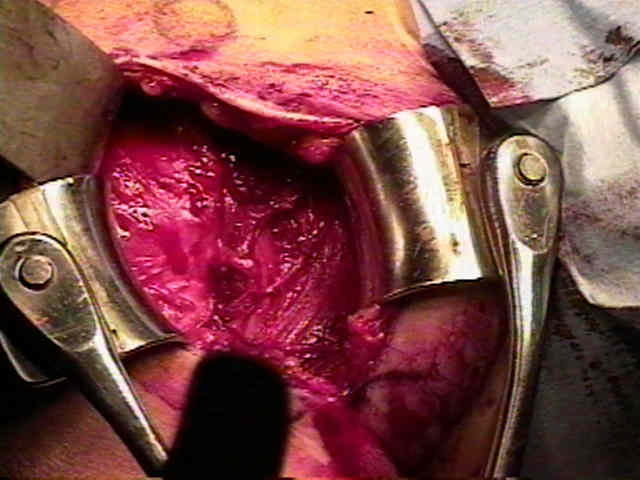
- Clavipectoral Fascial Incision:
- once the deltopectoral interval has been fully developed, the clavipectoral fascia is exposed (which is most prominent lateral to coracoid muscles);
- clavipectoral fascia is differentiated from the deeper tissues, because it will not move with internal and external rotation;
- tip of the coracoid and the conjoined tendon (short head of biceps and the coraco-brachialis) is identified;
- clavipectoral fascia is then divided vertically just lateral to the conjoined tendon, up to coracoacromial ligament, exposing subscapularis tendon & lesser tuberosity.
- proximally, the fascia is divided at a point just lateral to the coracoid;
- the incision is carried distally to the level of the anterior circumflex;
- these vessels mark the level of the subscapularis tendon;
- identification of musculocutaneous:
- musculocutaneous nerve can usually be palpated on deep surface of coracobrachialis;
- nerve enters posterior of coracobrachialis about 5 cm distal to coracoid tip but can be as close as 1 to 2 cm;
- retraction:
- often a "Charnley type" of self retaining retractor is inserted underneath the deltoid medially and the coracobrachialis laterally;
- coraco-acromial ligament:
- in patients w/ traumatic arthritis or DJD, the shoulders may be tight and therefore, the ligament can be partially incised for better
exposure of the upper portion of the subscapularis;
- in patients w/ rheumatoid arthritis or cuff tear arthropathy, excision of the CA ligament may destabilize the shoulder arthroplasty;
- Pectoralis Tendon:
- in some cases, it is necessary to detach the upper 1-2 cm of the pectoralis major tendon inorder to better visualize the capsule;
- this provides better visualization of inferior capsule & axillary nerve, which passes just inferior to the capsule;
- Sub-Detoid Space:
- elevate deep surface of deltoid (sub-deltoid bursa);
- laterally this will enter into subacromial bursa;
- the biceps tendon should now be exposed (internally rotate arm);
- at times the medial edge of the deltoid is covered by clavi-pectoral fascia, in which case, it should be sharply transected, to allow entry to the sub-deltoid space;
- Conjoined Tendon:
- once the deltopectoral interval has been fully developed, the clavipectoral fascia is exposed (which is most prominent lateral to coracoid muscles);
- tip of the coracoid and the conjoined tendon (short head of biceps and coraco-brachialis) is identified (the fascia edge is often more lateral than is often thought);
- the lateral edge of the clavipectoral fascia is differentiated from the deeper tissues, because it will not move with internal and external rotation;
- clavipectoral fascia is then divided vertically just lateral to the conjoined tendon, up to coracoacromial ligament, exposing subscapularis tendon & lesser tuberosity.
- Deep Retraction:
- identify the coraco-acromial and coraco-humeral ligaments;
- the coraco-humeral ligament is best identified w/ the arm in external rotation as the ligament passes on to the tuberosities;
- the CA ligament can be released but many surgeons will preserve the coracohumeral ligament, so that it can serve as a superior anchor for vertical capsular shift;
- prior to placement of retractors, it is necessary to indentify musculocutaneous nerve which usually lies just medial to the conjoined tendon and muscle;
- in the report by EG McFarland et al, the authors examined the relationship of the brachial plexus to the glenoid and the subscapularis muscle and evaluated the proximity of retractors used in anterior shoulder surgical procedures to the brachial plexus;
- 8 fresh-frozen cadaveric shoulders were exposed by a deltopectoral approach;
- subscapularis muscle was split in the middle and dissected to reveal the capsule beneath it;
- capsule was split at midline, and a Steinmann pin was placed in the equator of the glenoid rim under direct visualization;
- brachial plexus and axillary artery were within 2 cm of the glenoid rim, with the brachial plexus as close as 5 mm in some cases;
- there was no statistically significant change in the distance from the glenoid rim to the musculocutaneous nerve,
axillary artery, medial cord, or posterior cord with the arm in various degrees of abduction;
- retractors placed superficial to the subscapularis muscle or used along the scapular neck make contact with the brachial plexus in all positions tested;
- ref: The Anatomic Relationship of the Brachial Plexus and Axillary Artery to the Glenoid Implications for Anterior Shoulder Surgery



- next the Balfour Charnley type retractors are inserted;
- blades are placed deep to the deltoid and the conjoined tendon;
- inner limb of the Balfour should be just caudal to the coracoid tip;
- superior exposure if facilitated w/ a Chandler-Spade into subacromial space;
- alternatively consider use of the Mallon Retractor:
- Subscapularis Bursa:
- the subscapularis bursa is dissected off of the subscapularis tendon, w/ care to avoid damaging the underlying anterior humeral circumflex
arteryor its branches;
- Identification of the Musculocutaneous nerve
- Identification of the Axillary nerve
- Transection of the Subscapularis
- Caspsular Transection:
- external rotation of the humerus affords better capsular exposure and relaxes the nerve;
- insert a blunt retractor inferiorly to protect the axillary nerve, insert two single pronged skin hooks to elevate the capsule superiorly and
place it under tension; 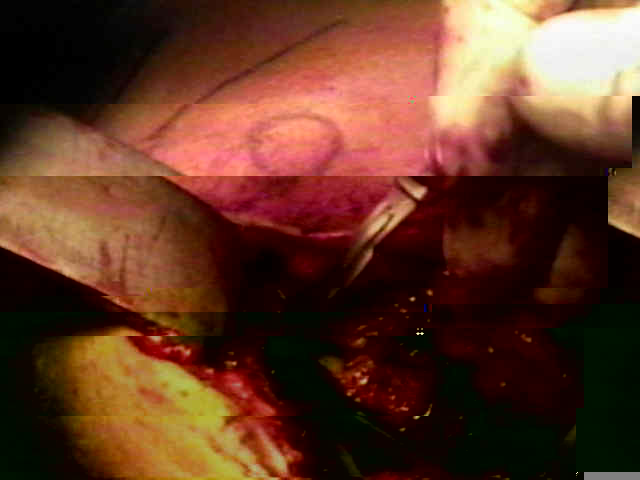
- vertically transect the capsule at a point midway between the lesser trochanter and the edgle of the glenoid;
- carry this vertical capsular incision superiorly into the rotator interval, which converts the capsular incision into a T
(since the rotator interval lies in a horizontal direction);
- at the end of the case, the superior and inferior capsular capsular flaps are closed (and shortened) in order to shift
the inferior capsule in a superior direction;
- the vertical portion of the incision is closed anatomically (so that there will be no loss of external rotation)