- Discussion: 
- shoulder arthroscopy / acute dislocations / recurrent anterior instability / multidirectional instability /
posterior instability
- drive through sign:
- refers to the ability to pass the arthroscope easily between the humeral head and the glenoid at level
of anterior band of inferior glenohumeral ligament;
- considered diagnostic of shoulder laxity or instability;
- ref: Clinical significance of the arthroscopic drive-through sign in shoulder surgery.
- arthroscopic findings:
- SLAP tear
- ALPSA lesion:
- may have higher chance of dislocation because these may heal medially on the scapular neck;
- Neviaser’s Contribution to the Treatment of ALPSA lesions
- Anterior labroligamentous avulsions lead to higher recurrent dislocations vs Bankart following arthroscopic repair
- Results of arthroscopic capsulolabral repair: Bankart lesion vs anterior labroligamentous periosteal sleeve avulsion lesion.
- glad lesion
- glenolabral articular disruption;
- lesion consists of an anterior-inferior labral tear associated with an injury to the glenoid articular cartilage;
- references:
- The glenolabral articular disruption lesion: MR arthrography with arthroscopic correlation.
- Anterior shoulder instability: MR arthrography in the classification of anteroinferior labroligamentous injuries.
- perthes lesion:
- variation of the Bankart lesion;
- lesion occurs when the scapular periosteum remains intact but is stripped medially
- torn anterior labrum is displaced only minimally
- Which labral lesion can be best reduced with external rotation of the shoulder after a first-time traumatic anterior shoulder dislocation?
- HAGL:
- The HAGL lesion: An arthroscopic technique for repair of humeral avulsion of the glenohumeral ligaments.
- Technique Considerations:
- preparation: considerations include need to document:
- completeness of the diagnostic examination
- adequacy of capsulolabral mobilization
- variation in the use of accessory portals
- use of additional capsular or labral plication or fixation.
- importance of portal placement:
- portals are as perpendicular as possible to the anterior glenoid surface (other wise there will be a tendency to
skive off of the osseous surface);
- in the case of a Bankart lesion, this may mean placing the anterior portal through the substance of subscapularis muscle;
- it is also important to keep the instrument portal as lateral as possible (again to be as perpendicular as possible);
- ref: Arthroscopic repair of anterior-inferior glenohumeral instability using a portal at the 5:30-o'clock position: analysis of the effects of age, fixation method, and concomitant shoulder injury on surgical outcomes..
- assesment:
- superior labrum (slap)
- remember that with significant (inferior instability) any superior labral tear will cause Superior GHL looseness;
- ref: Arthroscopic suture repair of superior labral detachment lesions of the shoulder.
- rotator interval lesion
- hill sachs lesion
- remplissage: partial transfer of infraspinatus into defect;
- ref: Anatomical and Functional Results After Arthroscopic Hill-Sachs Remplissage
- Anterior Bankart Repair / capsular shift;
- arthroscopic inferior capsular shift: (arthroscopic knots)
- surgeon establishes an antero-superior portal and a antero-inferior portal;
- arthroscopic graber is inserted through the superior portal and grasps the inferior capsule and then elevates this superiorly;
- guide wire (or hollow trochar - depending on the specific technique used), is passed through the elvated inferior capsule;
- this technique allows the surgeon to perform as much capsular shift as necessary in a controled fashion;
- anatomic considerations: rim angle is narrow over the anterior inferior glenoid and carefull drill placement is essential;
- references:
- Variations in glenoid rim anatomy: implications regarding anchor insertion.
- Anatomy of the axillary nerve and its relation to inferior capsular shift
- Arthroscopic glenohumeral folds and microscopic glenohumeral ligaments: the fasciculus obliquus is the missing link
- Arthroscopic Suture Anchor Capsulorrhaphy Versus Suture Capsulorrhaphy in a Cadaveric Model (SS-01)
- anchor insertion site:
- it is important to insert bone anchor right at the edge of the articular surface;
- if anchor drill hole is inserted slightly away from articular edge, there will be a tendency to skive off osseous surface;
- arthroscopic repair often tends to repair the torn labrum too medially (away from the glenoid rim);
- ref: Anchor Placement on the Glenoid Faceplate Does Not Improve Stability With Bankart Repair (SS-02)
- remplissage
- The Effect of Remplissage Procedure on Shoulder Stability and Range of Motion: An in Vitro Biomechanical Assessment
- Arthroscopic Bankart repair combined with remplissage technique for the treatment of anterior shoulder instability with engaging Hill-Sachs lesion: a report of 49 cases with a minimum 2-year follow-up.
- Anatomical and functional results after arthroscopic Hill-Sachs remplissage
- A prospective, comparative, radiological, and clinical study of the influence of the "remplissage" procedure on shoulder range of motion after stabilization by arthroscopic Bankart repair.
- Arthroscopic remplissage with Bankart repair for the treatment of glenohumeral instability with Hill-Sachs defects
- Outcomes of arthroscopic "remplissage": capsulotenodesis of the engaging large Hill-Sachs lesion.
- thermal shrinkage; (role unclear)
- Complications:
- recurrent instability;
- note that recurrent anterior instability + restriction of external rotation is a risk for not returning to high level sports;
- references:
- Revision of Failed Arthroscopic Bankart Repairs.
- Glenoid Rim Fracture After Anchor Repair. A Report of 4 Cases
- Arthroscopic revision Bankart repair: a prospective outcome study.
- Arthroscopic Bankart repair: results and risk factors of recurrence of instability
- Risk factors for recurrence of shoulder instability after arthroscopic Bankart repair
- axillary nerve injury;
- ref: Arthroscopic perspective of the axillary nerve in relation to the glenoid and arm position: a cadaveric study.
- complications from bone anchors:
- Osteolysis and Arthropathy of the Shoulder After Use of Bioabsorbable Knotless Suture Anchors. A report of four cases.
- Intraosseous foreign body granuloma in rotator cuff repair with bioabsorbable suture anchor.
- Glenoid osteolysis after arthroscopic labrum repair with a bioabsorbable suture anchor
- References:
Arthroscopic Treatment of Anterior-Inferior Glenohumeral Instability. Two to Five-Year Follow-up
Arthroscopic manifestations of shoulder subluxation and dislocation.
Effect of lesions of the superior portion of the glenoid labrum on glenohumeral translation.
Arthroscopic resection of glenoid labral tears in the athlete: a report of 29 cases.
Arthroscopic staple capsulorrhaphy for anterior shoulder instability.
Arthroscopic versus open Bankart procedures: a comparison of early morbidity and complications.
Arthroscopic Bankart suture repair: Technique and early results.
Arthroscopic Bankart suture repair.
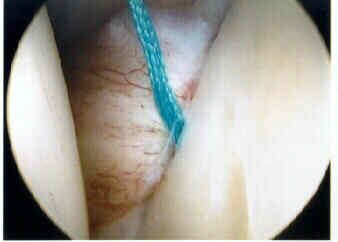
- case example:
- 35 year old male with anterior instability, w/ obvious drive through sign demonstrated at arthroscopy;
- arthroscopic grasper is inserted through the anterior-superior portal and is used to grasp the anteior-inferior capsule and to draw it superiorly;
- a suture passer is then inserted through the elevated capsule, which then sets up the Mitek knotless system