

- Discussion:
- this is probably an under rated procedure in terms of its indications;
- surgical indications:
- hallux valgus + 2nd toe amputation:
- great toe is stabilized in part by the presence of 2nd toe;
- when it is absent, a hallux valgus valgus deformity is best treated by arthrodesis of first MP joint;
- a soft tissue procedure will fail w/ time;
- failed Keller bunionectomy;
- young laborer w/ hallux valgus;
- arthrodesis provides best chance for long-standing painless joint;
- advanced degenerative changes:
- cheilectomy is not the procedure of choice in presence of advanced degenerative joint changes;
- rheumatoid arthritis:
- fusion is procedure of choice for hallux valgus assoc w/ advanced DJD, and a hallux valgus, advanced hallux valgus (IMA > 20 deg, HVA greater than 40 deg), severely subluxated or dislocated MTP joints, or for failed hallux valgus surgery;
- severe deformity:
- (IM angle > 20 degrees), an arthrodesis of MP joint may be used;
- arthrodesis is indicated in presence of severe subluxation or degenerative changes in metatarsophalangeal joint;
- Position of Arthrodesis:
- toe is placed in approx 25 to 30 degrees of dorsiflexion in relation to first metatarsal and approximately 10-15 deg of valgus in a first MP joint arthrodesis;
- first toe should end up resting comfortably against the second toe;
- toe should be in 15 deg of dorsiflexion from the floor (although during surgery it is not possible to make this determination);
- this places the least amount of stress on the interphalangeal joint of great toe & provides patient w/ smoother gait pattern.
- remember the angle of inclination to the floor helps fine tune the dorsiflexion; angle of MTP arthrodesis;
- a flat foot will need less dorsiflexion while a high arched foot will need more dorsiflexion;
- following arthrodesis, reduction of intermetatarsal angle will occur in proportion to the preoperative intermetatarsal angle;
- Technique:
- use standard medial approach to MTP joint;
- widely strip the capsule tissues both dorsally and plantarly, so that the joint is widely exposed;
- perform an excision of the medial exostosis; (see Silver procedure);
- use the exostosis as a source of bone graft;
- use a large towel clip to help hold the joint steady;
- use sharp currettes to remove the catilaginous and subchondral surfaces of the metatarsal and phalanx;
- attempt to shape the metatarsal into a rounded cone, while shaping the proximal phalangeal base into a symmetrically shaped rounded cup;
- remember that the cup and cone needs to be shaped to achieve optimal positioning of the metatarsal and phalanx;
- if the cup and cone have rounded surfaces, the phalanx can be rolled over the metatarsal to achieve a better position;
- consider drilling small holes in the MTP surfaces to promote bony ingrowth;
- note: w/ a rheumatoid forefoot which requires a Hoffman procedure consider shortening the distal metatarsal so that 1st MP segment will maintain a normal cascade in relation to the other MTP segments;
- Insertion of Hardware:
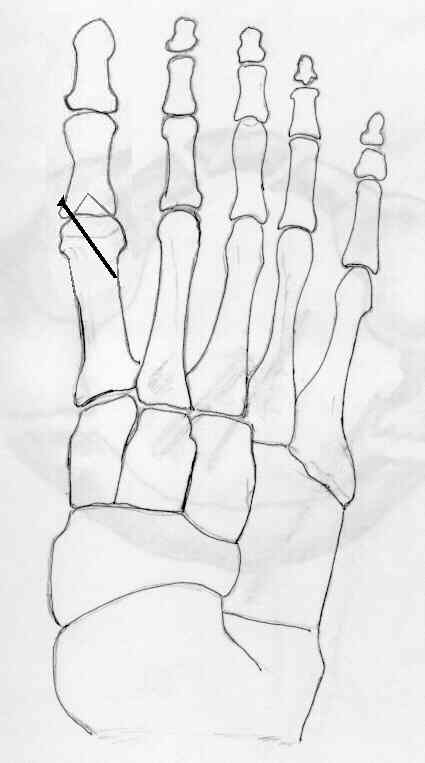
- w/ good bone stock consider using a single 4-0 cannulated screw;
- insert the K wire just proximal to the flare of medial base the proximal phalanx;
- if the K wire is inserted down the medullary canal, then a cancellous screw will be required;
- if the K wire is inserted into the lateral aspect of the metatarsal then a cortical screw is required;
- check MTP joint position prior to tapping and inserting the screws;
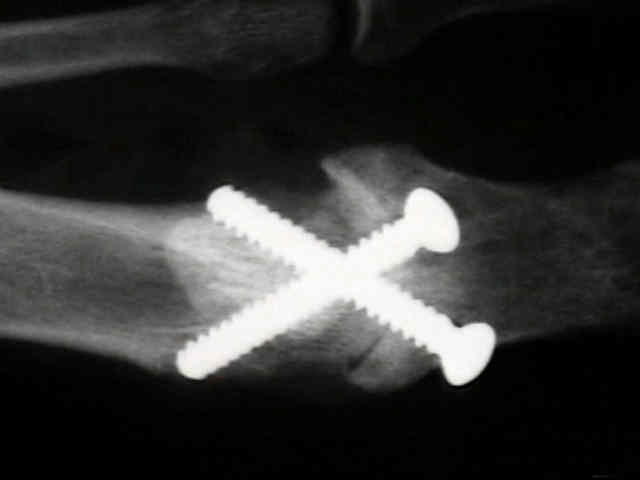
- w/ poor bone quality, as in rheumatoid arthritis, consider use of crossed K wires (or small threaded Steinman pins) for a period of 4-6 weeks;



- Bone Graft:
- examine intra-operative radiographs (or flouro) for areas of partial bone separation;
- any areas of bone separation should be filled in with bone graft from the exostosis;
- consider need for mini iliac crest graft harvest in patients that smoke heavily;
- Post Op:
- non weight bearing in a cast for 6 weeks, depending on radiographic results;
- once fusion mass is mature, patients may find shoe wear somewhat limited, especially with regard to heel height;
- in some cases, patients may prefer a rocker bottom type of sole;
- Complications:
- complications include malunion, non union, and IP DJD (develops after the fusion);
- excessive dorsiflexion will cause the IP joint to rub in the shoe;
- in this case, the IP joint may begin to claw, and shoe wear will be restricted;
- insufficient plantar flexion, will cause lateral roll off or vaulting gait
Hallux rigidus and osteoarthrosis of the first metatarsophalangeal joint.
Arthrodesis of the first metatarsophalangeal joint.
Arthrodesis of the first metatarsophalangeal joint as salvage for the failed Keller procedure.
Metatarsocuneiform arthrodesis for management of hallux valgus and metatarsus primus varus.
Arthrodesis of the first metatarsophalangeal joint for hallux valgus in rheumatoid arthritis.
Compression-screw arthrodesis of the first metatarsophalangeal joint of the foot.
Arthrodesis of the first metatarsophalangeal joint.
Related Products
Roll-A-Bout
An alternative to crutches and wheelchairs. The Roll-A-Bout fully supports the lower leg guaranteeing 100% non-weight-bearing.