

- See: Hetertopic Ossification of the Elbow:
- Discussion:
- most indicated for flexion contractures of the elbow (w/o extension contracture);
- disadvantages:
- some patients may gain extension but will loose flexion (especially if they are casted in extension);
- possible wound dehiscence from tension on the anterior soft tissues;
- inability to address the posterior structures;
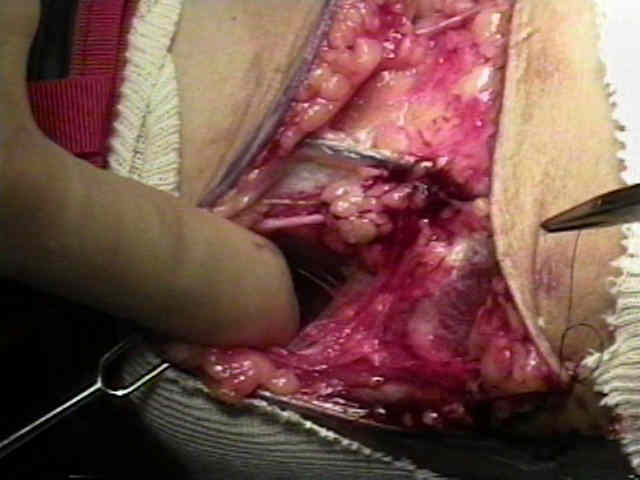
- Incision:
- oblique transverse incision is made extending across the antecubital fossa
- insision is carried obliquely and proximally along the radial aspect of the arm, a distance of 5-6 cm;
- incision is carried obliquely distally along the medial aspect of the arm, a distance of 5-6 cm;
- incision is carried thru subQ tissues, with care to avoid injury to superficial veins, and the medial and lateral antebrachail cutaneous nerves;
- it is necessary to develop full thickness subcutaneous flaps for adequate exposure;
- lacertus fibrosis of the biceps is incised, which allows subsequent exposure of the the median and ulnar nerves;
- Deep Dissection:
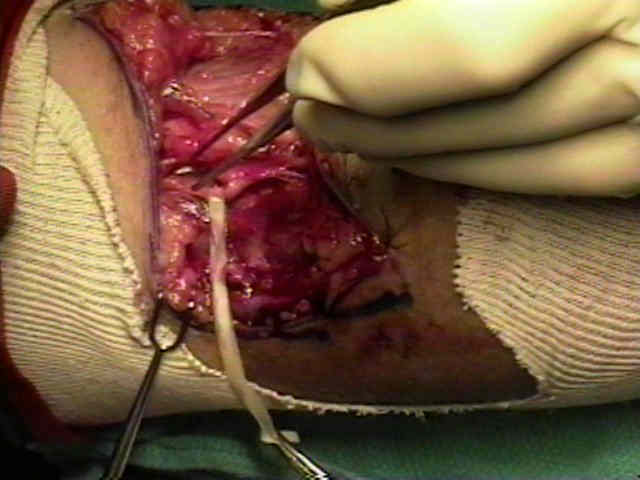
- identification of radial nerve;
- radial nerve is identified between the brachioradialis and brachialis;
- nerve is tagged with a rubber dam;
- during the procedure the nerve is retracted laterally w/ a thyroid retractor;
- identification of median nerve and brachial artery
- both the median nerve and brachial artery are tagged w/ rubber dam;
- the deep dissection procedes medial to the N/V bundle;
- the nerve and artery will be gently retracted laterally during the case w/ an appropriately sized thyroid retractor;
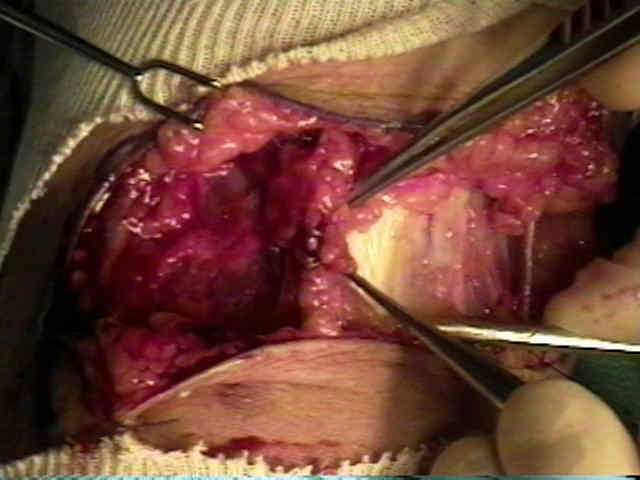
- identification of joint capsule:
- use a kitner rolled up sponge (peanut) to gently sweep the remaining soft tissues off the joint capsule (which is white compared to the other tissues);
- begin at the most medial aspect of the capsule and proceed to sweep the overlying tissues off the capsule in a radial direction;
- flexion and extension of the joint will help keep the dissection over the most central portion of the dissection;
- the coronoid process process is another useful landmark;
- once the dissection becomes difficult due to the overlying biceps and brachialis, then begin to sweep the soft tissues off the
capsule (using a peanut) starting at the most radial aspect of the joint and then proceding medially;
- if there is any question of the level of the capsule, pass a right anlge retractor along the capsule from a
medial to radial direction and then locate the tip of the right angle thru the lateral windon;
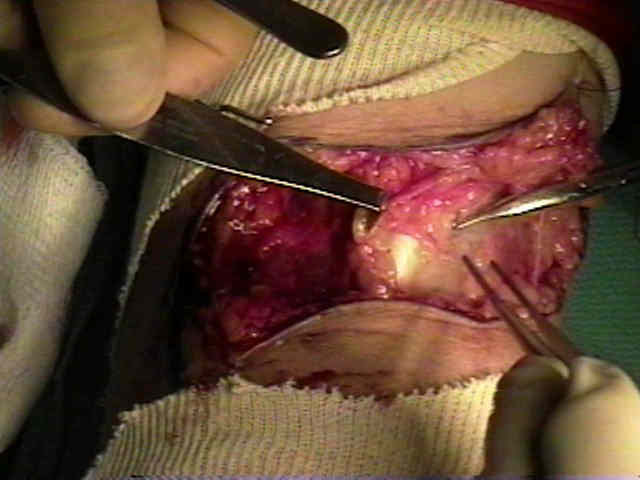
- transection of the capsule
- prior to transection of the capsule, their should be a clear view of the capsule from both the medial and lateral directions;
- flex and extend the elbow to identify the center of the capsule;
- use a 15 blade scapel to transect a window of the capsule from the medial to the lateral edges of the capsule;
- it is essential that the dissection begn as far medially as possible w/o injuring the MCL;
- the medial tongue of capsule is grasped w/ a clamp and is passed into the lateral window;
- laterally the dissection needs to procede past the radial head;
- Manipulate Elbow:
- gentle extension force is applied to the elbow;
- Post Op:
- the elbow can be splinted in extenion for one week prior to ROM;
- Case Example by Dr James R. Urbaniak MD: 






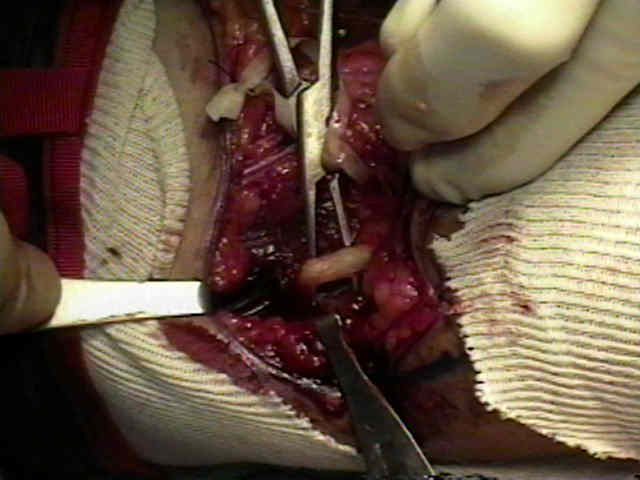
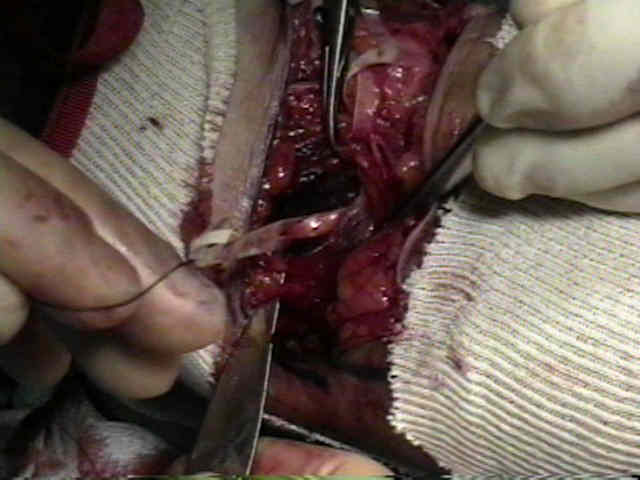
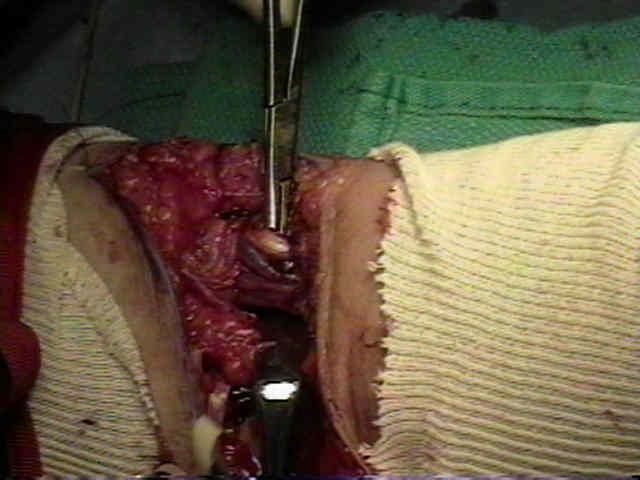


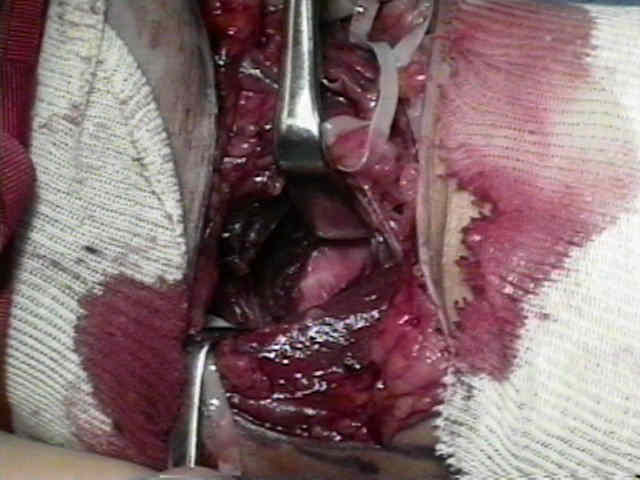
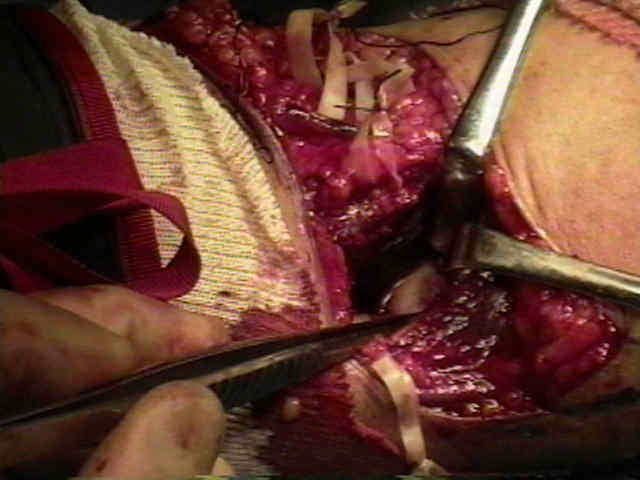

Correction of post-traumatic flexion contracture of the elbow by anterior capsulotomy.