

 - See
- See
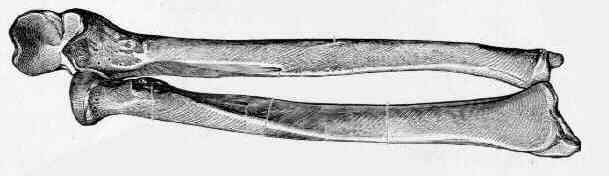
- Pediatric Both Bone Frx
- Deforming Forces
- Discussion of Blount Fractures
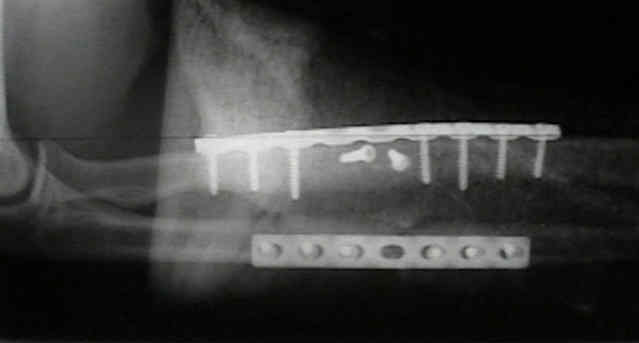
- Implants for Fractures of the Radius and Ulna
- Plating Techniques
- Indications for Operative Treatment:
- all displaced, unstable fractures of the radius and ulna in adults;
- radial shaft fractures: all displaced fractures of the radius with greater than 10 deg of angulation or w/ subluxation of proximal
or distal R-U joint
- ulnar shaft fracture: isolated frxs of the ulna with angulation greater than 10 deg;
- Exam Considerations:
- forearm compartment syndrome
- references:
- Acute compartment syndrome of the forearm
- Pre Op Planning:
- tourniquet:
- open fractures: (see Gustillo Classification)
- open fractures should be treated as an emergency, but fixation may be delayed upto 24 hrs;
- immediate ORIF in grade I, II, and IIIa fractures can have good results (low infection rate);
- autogenous bone grafting can be carried out early for grade I and II fractures (if needed);
- grade IIIb and IIIc fractures had poor results;
- these fractures were serially debrided until judged clean, only at which time was bone grafting performed;
- despite these measures, infections may occur in upto 3/4 of these patients;
- wound closure:
- some surgeons will close surgical incisions, where as, traumatic wounds are left open and are closed by delayed suture at a
second or third look debridement;
- 2 days of antibiotics should follow each wound debridement;
- consider antibiotic bead pouch between debridements;
- references:
- Immediate internal fixation of open fractures of the diaphysis of the forearm.
- The necessity of acute bone grafting in diaphyseal forearm fractures: A retrospective review.
- Surgical Approach:
- Approach to the Ulna
- Anterior Approach: (Henry);
- main disadvantage is postoperative finger stiffness due to stripping of FDS/FPL origin;
- Dorsal Approach (Thompson):
- main disadvantage is possible injury to the posterior interosseous nerve;
- Surgical Reduction:
- both frx are exposed and provisionally reduced before either fixation is completed;
- the frx that has the least comminution (usually the ulna) is fixed first;
- if reduction is impossible the plate on the other bone is loosened and second bone reduced;
- after reduction and provisional fixation of both bones, pronation and supination are examined (if OK, all the screws are inserted);
- comminution and segmental bone loss:
- comminution makes it difficult to restore bone to length;
- interosseous membrane is identified, proximally & distally, & used guide in restoring bones to adequate length;
- bone grafting:
- it is generally recommended that bone grafting be applied to both bone forearm fractures w/ more than 50% comminution;
- indications for bone grafting have recently been challenged by Wright et al 1997, who were unable to find any
advantages to bone grafting in a retrospective review of 198 both bone fractures;
- if bone graft is used, it should be away from interosseous membrane to decrease risk of synostosis (this complication is
more common in head injured patients);
- refs:
- The management of segmental bone loss associated with forearm fractures.
- Comminuted fractures of the proximal radius and ulna.
- Cross-union complicating fracture of the forearm. Part I: Adults.
- The necessity of acute bone grafting in diaphyseal forearm fractures: A retrospective review.
- Fracture-related and implant-specific factors influencing treatment results of comminuted diaphyseal forearm fractures without bone grafting.

- Wound Closure:
- closure of both incisions without tension may be difficult;
- ulnar would should preferably be closed first, since it is located close to the subcutaneous border;
- radial wound, however, can be left open over a portion of its length, if the metal implant is safely placed under the muscle;
- Post Operative Care, Complications, and Evaluation
Forearm fractures: treatment by rigid fixation with early motion.
Long-term follow-up of forearm bone diaphyseal plating.
Operative treatment of malunited fractures of the forearm.
Immediate internal fixation of open fractures of the diaphysis of the forearm.