

Co-authored by: Jan Van Der Bauwhede MD
- Discussion:
- disorder of unknown etiology characterised by local proliferation of abnormal fibrous tissue in the plantar fascia
- this tissue is locally aggressive and progressively replaces the normal plantar aponeurosis
- this leads to often painful thickened fascia with nodules from 0,5-3 cm in diameter
- may also infiltrate the dermis or very rarely the flexor tendon sheath (flexion contracture of 2nd toe)
- age range from childhood until 6th decade, more common in men than in women
- 25 % of patients have bilateral involvement
- in older people sometimes associated to other fibromatoses like Dupuytren's in the hand or La Peyronie's disease,
a fibrous infiltration of the corpora cavernosa
- increased incidence in patients with:
- diabetes mellitus
- seizure disorders
- Pathoanatomy:
- the histological and ultrastructural features of Ledderhose and Dupuytren's disease are the same
- this supports the hypothesis that they have a common etiology and pathogenesis
- features1
- nodules: tightly packed fibroblasts, small amount of extracellular matrix
- cords: mainly extracellular matrix, less tightly packed elongated fibroblasts parallel to the main axis of the cords
- in children the histological aspect might be mistaken for malignant fibrosarcoma2
- Diff dx:
- traumatic partial fascia rupture
- neurilemmoma or schwannoma
- lipoma
- neurofibroma
- History/Exam:
- nodule or nodules on the medial plantar aponeurosis
- may be painful with ambulation
{kind=link}



- Non Operative Treatment:
- small nodules causing no pain can be left alone3
- pain reduction and long term relief of symptoms can be obtained using:
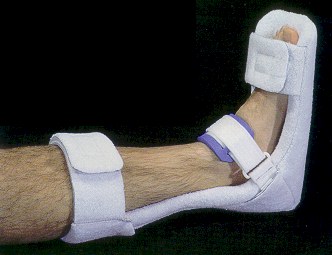
- night splints (adding a great toe wedge will increase stretching effect
on fascia, but can be very painful in the beginning)
- a plantar fascia stretching device
- orthotics and shoe wear modification
{kind=link}
- Expected Results with Surgery:
- high incidence (57 %) of local recurrence when only fibroma is removed4
- Indication/Contraindication for Surgery:
- indication:
- large nodules causing pain or nerve compression, with no improvement by stretching/splinting/shoe wear modification
- contraindication:
- bad vascular status of foot (vascular disease, microvascular disease)
- Surgical Approach: wide resection of nodules + surrounding macroscopically 'normal' fascia
- longitudinal incision along medial-plantar aspect of first metatarsal (Pederson and Day)5
- proximally to the tarsal navicular
- development of skin flaps to expose the fibroma and fascia
- aggressive excision of lesion + normal appearing adjacent fascia
- tack down skin flaps to prevent hematoma
- close on suction tubes lying beneath the skin
- Postoperative Management:
- firm compression dressing
- protected weight bearing in postop shoe as soon as pain permits
- Recurrence:
- in case of recurrence and lots of pain: complete fascial excision
- References
1. De Palma L, et al. Ledderhose Disease: a histochemical and ultrastructural analysis. Eur Foot Ankle Soc Congress, Paris, October 23-25, 1997, Abstract 85
2. Juvenile aponeurotic fibroma. Report of three cases and a review of the literature.
3. Mann RA, Coughlin MJ. Plantar Fibromatosis. Surgery of the Foot and Ankle, 6th ed. Mosby-Year Book, Volume 2, 994-995.
4. Lutter LD, Mizel MS, Pfeffer, eds. Plantar Fibromatosis. Orthopaedic Knowledge Update. Foot and Ankle. American Orthopaedic Foot and Ankle Society. p.23, 1994.
5. Pederson HE, Day AJ. Dupuytren's Disease of the Foot. J Am Med Assoc. 1954;154:33.
Gigante A, Carloni S, de Palma L. Cell and Extracellular Matrix in Dupuytren's Disease. 3d Congress EFORT, Barcelona, Spain, April 24-27,1997, P056
Plantar fibromatosis: an isolated disease.
© C.R. Wheeless - J. Van Der Bauwhede