

- See: Total Hip Replacement Menu
- Discussion:
- most common complication in total hip arthroplasty and most common cause of component failure;
- osteolysis is a time dependent process which arises from inflammatory reaction against polyethylene particulate debris;
- patho-biology:
- osteolysis is mediated primary by macrophages (fibroblasts and endothelial cells also play a role);
- these cells are activated by wear debris (primarily polyethylene, but also metal and polymethylmethacrylate debris);
- chemical mediators include: interleukin-1 (bone-resorbing cytokine) and tumor necrosis factor;
- in the report by Bi Y, et al (2001), the authors present study showed that titanium particles induced both murine marrow cells and human peripheral blood monocytes to produce factors that stimulated osteoclast differentiation;
- mean increase in osteoclast differentiation was 29.3 ± 9.4-fold.
- they showed that titanium particles stimulate in vitro bone resorption primarily by inducing osteoclast differentiation;
- ref: Titanium Particles Stimulate Bone Resorption by Inducing Differentiation of Murine Osteoclasts
- systemic effects:
- main concern involves dissemination of wear particles to the liver, spleen, and abdominal lymph nodes of THR patients;
- debris can be demonstrated in the fixed macrophages and Kupffer cells lining the hepatic sinusoids;
- role of ceramic bearing surfaces:
- ceramic bearing surfaces have offered hope in some series of decreasing osteolysis by minimizing wear debri;
- it is noted that alumina ceramic provides an ultra smooth surface (compared to metal on polyethylene);
- in the series by Yoon TR (1998), 103 hips had insertion of the ceramic head and acetabular component;
- at mean duration of 92 months, femoral osteolysis occured in 23 hips and acetabular osteolysis occured in 49 hips;
- in patients who underwent revision for osteolysis, abundant ceramic wear particles;
- the authors cited caution with this type of component noting the high rate of failure;
- references:
- Osteolysis in association with a total hip arthroplasty with ceramic bearing surfaces.
- Femoral Osteolysis:

- endosteal, intracortical, or non-linear cancellous bone destruction;
- in contrast, loosening will tend to demonstrate progressive linear radiolucency;
- mechanism of osteolysis:
- wear debris migrates down medullary canal between bone-cement (or press fit interface) following path of least resistance;
- intracapsular pressure may be a driving force;
- poorly fitting components may accentuate accumulation of wear debris down the medullary canal;
- do cemented femoral stems show less osteolysis that press fit stems?
- some authors postulate that cement is a more reliable barrier to migration of wear debris down the medullary canal as compared
to press fit components;
- depending on the data being examined, osteolysis may occur in up to 10-30% of femoral stems inserted without cement as compared to a prevalence of 1-2% using modern cementing techniques;
- w/ press fit designs some authors feel that circumferential press fit stems offer more reliable protection against wear debris as compared to non circumferential designs;
- porous coating may provide a barrier to migration of wear debris;
- references:
- Polyethylene wear and calcar osteolysis.
- Patterns of osteolysis around total hip components inserted with and without cement.
- Studies of the mechanism by which the mechanical failure of polymethylmethacrylate leads to bone resorption.
- Measurement of Polyethylene Wear in Acetabular Components Inserted with and without Cement. A randomized trial.
- Effect of Circumferential Plasma-Spray Porous Coating on the Rate of Femoral Osteolysis After Total Hip Arthroplasty.
- Acetabular Osteolysis:
- acetabular osteolysis is generally asymptomatic and may occur regardless of whether the component is well fixed;
- because osteolysis is asymptomatic, it is necessary to obtain periodic radiographs;
- note that acetabular osteolysis often will only be evident on oblique radiographs;
- as noted by Devane et al. (1997), osteolysis was associated with an increased rate of polyethylene wear only in hips that were inserted w/o cement;
- as noted by Bohm and Bosche (1998), the 11 year survivorship of press fit Harris Galante components was 97.7%;
- there was only one case of osteolysis in this study;
- holes in the acetabular component did not correlate with pelvic osteolysis;
- note that the majority of femoral heads in this study were made of ceramic;
- management: revising the component:
- main risks include probability that there will be major bone loss during implant removal;
- surgeon should be prepared to re-insert a much larger acetabular component following component removal;
- ref:
- Measurement of Polyethylene Wear in Acetabular Components Inserted with and without Cement. A randomized trial.
- Survival analysis of the Harris-Galante I acetabular cup.
- Noncemented acetabular component removal in the presence of osteolysis: the affirmative.
- management: leaving the component in place:
- this avoids all of the complications of implant removal and re-insertion;
- main disadvantage is limitation of exposure (limitation of debridement and bone grafting);
- if the area of osteolysis is central then consider curretage and bone grafting through the component screw holes (if these are present);
- if the area of osteolysis is superior or peripheral, consider making an osseous window to gain access to the lesion;
- in the study by Maloney et al (1997), 35 THR patients w/ porous acetabular components demonstrated acetabular osteolysis;
- these patients were managemed by liner removal, debridement of the osteolytic defect and bone grafting, followed by liner exchange;
- after an average of 3 years, the bone grafts had appeared to consolidated and no progressive bone erosion was seen;
- as noted by Schmalzried, et al (1998), osteolysis was successfully managed by leaving well fixed components in place and by working around the component (either thru the component holes or around the perimeter) inorder to currett out the osteolytic lesion;
- maximum size of lesions was about 7 x 5 cm;
- defects were filled with autograft or allograft;
- non of the osteolytic lesions were noted to progress after an average of 40 months;
- controversies:
- fosfamax: some evidence that this can reverse the effects of osteolysis;
- references:
- Treatment of pelvic osteolysis associated with a stable acetabular component inserted without cement as part of a total hip replacement.
- The fate of pelvic osteolysis after reoperation. No recurrence with lesional treatment.
- Survival analysis of the Harris Galante I acetabular cup.
- Improving the detection of acetabular osteolysis using oblique radiographs.
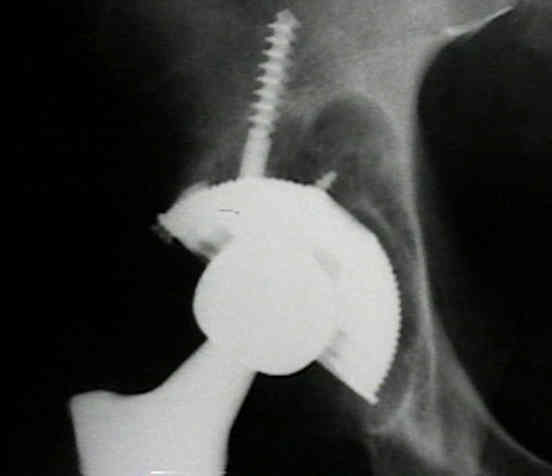
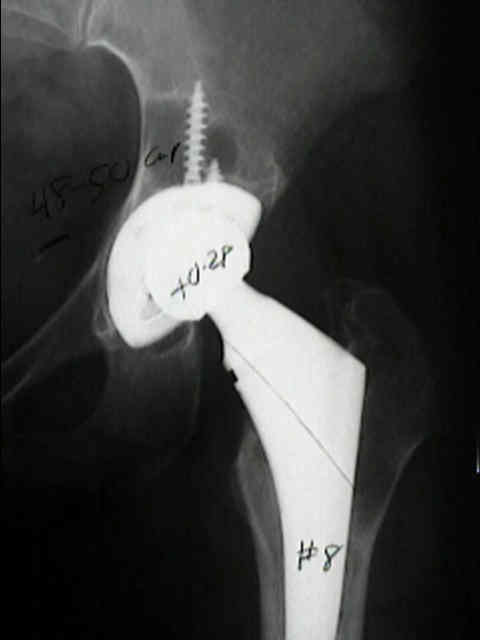
- Case Example:
- 50 year old patient w/ a well placed acetabular cup (against the tear drop) and well placed femoral stem;
- after 7 years, the patient has developed extensive osteolysis;

- Cemented Acetabular Component:
- 60 year old patient w/ a Charnley Muller THR which has done well for over 15 years;
- note that there is no acetabular osteolysis;

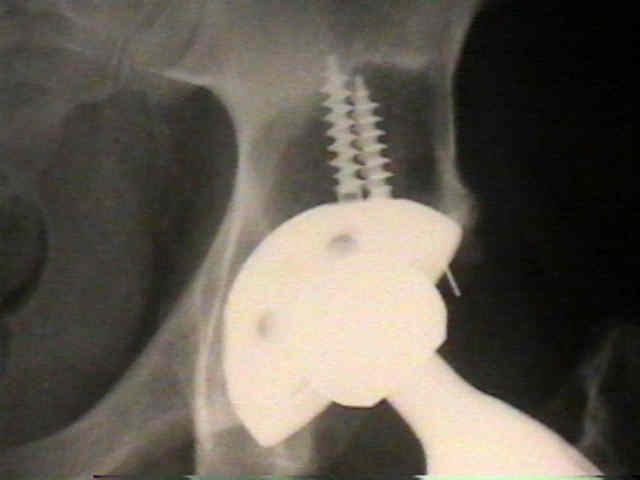
- Case Example:
- note that a large cup was used on this patient's left side (no osteolysis) where as a smaller cup was used on the right side (significant osteolysis is present at 7 years postop)


Localized osteolysis in stable, non-septic total hip replacement.
Aggressive granulomatous lesions associated with hip arthroplasty. Immunopathological studies.
Isolation and characterization of debris in membranes around total joint prostheses.
Wear of the polyethylene of Harris-Galante acetabular components inserted without cement.
Localized osteolysis in stable, non-septic total hip replacement.
Debris from cobalt-chrome cable may cause acetabular loosening.
Resorption of bone by inflammatory cells derived from the joint capsule of hip arthroplasties.
Patterns of osteolysis around total hip components inserted with and without cement.
Cellular biology of bone-resorbing cells.
Magnetic Resonance Imaging After Total Hip Arthroplasty: Evaluation of Periprosthetic Soft Tissue.
Nonsurgical Management of Osteolysis: Challenges and Opportunities.
The Value of Anteroposterior Pelvic Radiographs for Evaluating Pelvic Osteolysis.
Progression of Periacetabular Osteolytic Lesions
Pathophysiological Aspects of Hip Implants from the Orthopaedic Care Textbook
Transient Osteoporosis of the Hip from the Orthopaedic Care Textbook