Tom Large, MD
Ben Kam, MD
A. Define the spectrum of injury
I. Mechanisms
A. Combat/disaster injuries often via high energy mechanisms and of magnitude not frequently seen in everyday civilian sector
1. improvised explosive devices (IEDs)
2. land mines
3. rockets or rocket-propelled grenades (RPGs)
4. mortars
5. collapsing structures and flying debris (in natural disasters)
B. Blast, penetrating, or crushing injury pattern to soft tissues is well described and injuries may result from
1. primary pressure wave
2. secondary flying debris and bomb fragments
3. tertiary propulsion of individuals from blast wind
4. quaternary mechanisms, such as collapsing structures or burning materials
C. Lower energy mechanisms also possible and would result in closed fractures or smaller soft tissue injuries
II. Injury Patterns
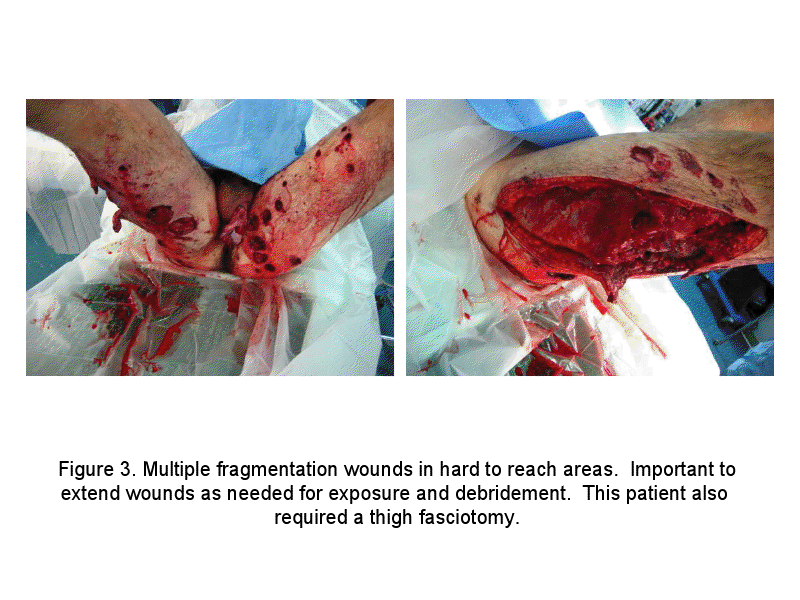
A. Peppering/fragmentation-type shrapnel injuries
B. Isolated soft tissue wounds
C. Isolated closed or open fracture on single extremity
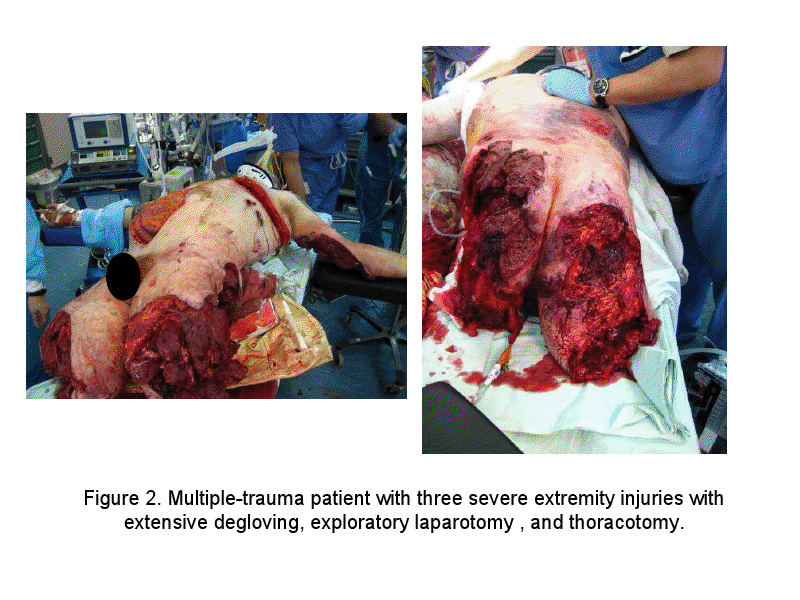
D. Multiple extremity injuries with any combination of open fractures, traumatic amputations, or large soft tissue wounds, including associated thermal/burn injury
E. Multi-trauma patients – any of the above injuries with concomitant vascular, nerve, head, chest, or abdominal injuries are usual
G. Associated soft tissue injuries can be large and grossly contaminated with debris
H. Blast mechanism or high energy gun shot wound allow for possibility of a relatively innocuous-appearing entrance wound associated with a large amount of underlying nonviable tissue and extensive foreign material contamination
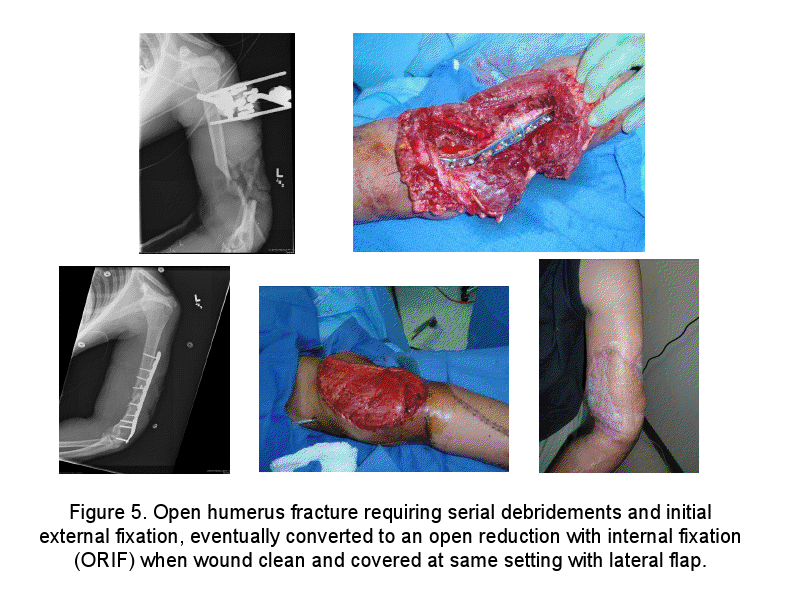
I. Due to high energy nature of these injuries, nearly all open fractures are Gustilo Anderson type IIIA, IIIB, or IIIC injuries
J. Distribution of these injuries can be important – wounds to limbs predominate most historical accounts of battle injuries among those surviving their wounds
|
|
Total Percentage of Injuries1
|
|
Conflict
|
Head/ Neck
|
Thorax
|
Abdomen
|
Limbs
|
Other & Multiple Injuries
|
|
World War I (Western Allies)
|
17
|
4
|
2
|
70
|
7
|
|
World War II (Western Allies)
|
4
|
8
|
4
|
79
|
9
|
|
World War II (USSR)
|
19
|
9
|
5
|
67
|
0
|
|
Korea (USA)
|
17
|
7
|
7
|
67
|
2
|
|
Vietnam (USA)
|
14
|
7
|
5
|
74
|
0
|
K. Of those who sustain lethal conflict/battle wounds, central wounds predominate – wounds to head or chest predominate these casualties
|
Area of injury1
|
U.S. fatalities in WWII
|
U.S. fatalities in Vietnam
|
Israeli fatalities in Lebanon ‘91
|
|
Head/neck
|
42%
|
46%
|
34%
|
|
Chest
|
30%
|
24%
|
45%
|
|
Abdomen
|
12%
|
9%
|
|
|
Multiple injuries
|
|
17%
|
|
|
Limbs
|
13%
|
3%
|
21%
|
|
Soft tissue
|
|
1%
|
|
L. Nature of conflict/disaster has significant impact on expected wounding/injuries
1. urban earthquake – crush from debris/buildings may predominate
2. rural conflict – gunshot and penetrating knife wounds may predominate
3. terrorist explosive event – blast/fragmentation injury may predominate
M. Mortality in civilian trauma was characterized by D. Trunkey in 1983 as having a trimodal distribution4
1. Peak 1: immediate deaths occur within moments of injury from overwhelming injury to vital structures (brain, heart, lungs)
2. Peak 2: Early deaths occur within minutes to hours following trauma, many due to exsanguinating hemorrhage, impaired breathing from survivable head injury, and compromised breathing from pneumothorax
3. Peak 3: Late deaths occur within days to weeks from trauma as result of complications of initial injury (multi-organ failure, infection, uncontrolled cerebral edema, etc.)
III. Early Evaluation
A. Often, early in conflict/disaster, demand for tertiary level medical care will exceed availability
B. In these settings, essential to have system of medical/trauma triage and to answer some key questions
1. if resources limited, who should receive priority?
2. can care be safely rendered at battle site/place of disaster?
3. is there land, sea, or aeromedical evacuation capability?
C. Always remember to focus team on saving life first, then limb-threatening injuries
D. Early involvement of orthopedic surgeon as part of a multi-disciplinary trauma team is essential to triage urgency of surgical interventions to multiple-injured patient
E. With healthy relationship and respect for colleagues, often possible to begin stabilizing fractures and debriding wounds on extremities while trauma surgeons perform exploratory laparotomy or vascular surgeon explores wound on different limb
IV. Lessons of Clinical Significance from the International Red Cross Manual on War Surgery1
A. Wounds to head and torso are most lethal – most survivors have extremity injuries, which compose majority of surgical workload and morbidity
B. Lethality of penetrating head wounds is 75%, despite fact that head represents only 9% of exposed body surface area
C. Uncontrolled exsanguinating hemorrhage accounts for some 50% of deaths
1. some 80% are central thorax or abdominal injuries, which require surgical care
2. some 80% of chest wounds can be managed with tube thoracostomy
D. Other 20% of hemorrhage deaths are due to extremity peripheral vessel injury
E. Some immediate and early deaths can be prevented by personal body armor covering the torso
F. Many early deaths can be prevented by
1. control of limb hemorrhage and aggressive management of shock
2. relief of airway obstruction
3. relief of tension pneumothorax
4. early medical evacuation to surgical treatment facility
References
1. Giannou C. War Surgery, vol. 1. International Committee of the Red Cross, ICRC. May 2010, chapter 5, pp 95-125.
2. Nessen S, Lounsbury DE, Hetz SP. War surgery in Afghanistan and Iraq. Dept. of the Army: Borden Institute, 2008.
3. Pollak AN, Calhoun JH. Extremity war injuries: state of the art and future directions. J Am Acad Orthop Surg. 2006;14(10):S1-S213.
4. Trunkey DD. Trauma. Sci Am. 1983;249:220-227.
B. Describe the fundamental principles of wound management
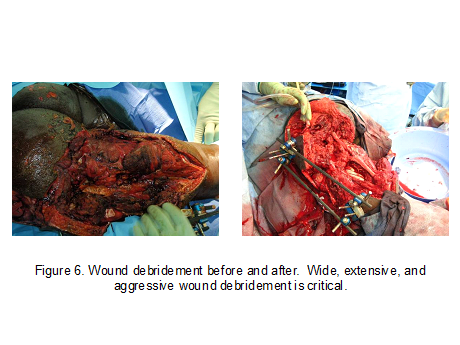
A. Meticulous wound management and aggressive debridement perhaps the most important service performed by orthopedic surgeon for combat/disaster injuries
B. All nonviable tissue should be excised and aggressive attempts to remove foreign material burden should be performed, including copious irrigation
C. Wounds should be adequately extended to expose zone of injury
D. Determining tissue viability can be difficult
1. helpful factors: color of tissue, contractility, whether tissue bleeds when cut
2. relatively straightforward determination of clearly viable and clearly nonviable tissue
3. “gray area” where tissue viability not clearly demarcated or determinable
a. tissue of questionable viability will usually declare itself to be devitalized at later debridement in 24-72 hours
b. aggressive early debridement of questionable tissue is prudent unless its preservation is of clinical importance (such as preserving important length or coverage to amputation or open fracture)
E. War/disaster wounds should never be closed primarily because of aforementioned issues with tissue viability and hidden foreign debris
F. Neurovascular structures, tendons, and joint surfaces should be carefully preserved by rotational coverage whenever possible
II. Foreign Material
A. Surgeon often faced with extensive embedded foreign debris or shrapnel
B. Debris exposed in base of wound should be meticulously removed
1. large wounds will usually allow access to debris via cavitary pockets created during injury (
see figure 9)
2. extending wounds to expose these cavitations is critical
C. In cases of small peppering shrapnel wounds, surgeon should not go on time-consuming “needle in haystack” search for isolated fragments
D. Any peppering entrance wound that allows entrance of standard size curette tip should be extended to allow debridement and irrigation
E. Superficial peppering injuries can be treated with curettage and scrubbing with surgical scrub brushes
F. Hunting for every fragment usually not necessary
G. Absolute indications for fragment excision
1. retained fragment in synovial joint
2. fragments causing compression of neuroaxis (spinal canal or brain)
3. fragments at risk for erosion or migration into vital structures
III. Irrigation
A. Normal saline irrigation used without additives
1. no benefit shown from addition of antibiotics
2. although some benefit from detergent additives shown, not routinely used
B. Pulsatile high-pressure lavage should be avoided as this may cause additional tissue damage or push debris deeper into wound
C. High flow, low pressure (gravity) irrigation using cystoscopy tubing preferred (
see figure 10)
D. 9 L – preferred volume of irrigation for each open wound
E. Irrigation as early as possible after injury shown to be beneficial
IV. Wound Vacuum-Assisted Closure (VAC)
A. Wound VAC is preferred wound dressing
1. care should be taken to ensure good seal and well-functioning VAC
2. patients to be evacuated may be indicated for smaller Freedom VAC (approved for use on military aircraft) (
see figure 11)
B. Care should be taken to obtain coverage with muscle or fascia over named vascular structures prior to VAC application
1. if this cannot be achieved, or seal cannot be obtained, standard wet-to-dry dressing can be used
2. if possible, change wet-to-dry dressing every 6 hours
V. Prevention of infection. Guidelines updated in an August, 2001 Journal of Trauma Supplement. Highlights of these recommendations:
A. Antimicrobials should be given as soon as possible. Initiation within three hours of injury may lower infection rates.
B. The choice and breadth of antibiotic coverage also remains controversial. 2g IV cefazolin q6-8hrs for 24-72 hours is the current recommendation. Fluoroquinolones and aminoglycosides were previously recommended to enhance gram negative coverage; this is no longer the case. Similarly, adding penicillin as clostridial or streptococcal coverage is no longer recommended.
C. Negative pressure wound therapy and/or antibiotic bead pouches should be considered.
D. Routine surveillance cultures of traumatic open fracture wounds are controversial. Positive cultures have been predictive of ultimate infection rates and are a risk factor for an amputation. However surveillance cultures are rarely predictive of the infecting organism and cannot be recommended as a guide to initial antibiotic choice at this time
References
Burns TC, Stinner DJ, Mack AW et al. Microbiology and injury characteristics in severe open tibia fractures from combat.
J Trauma. 2012;72:1062-7.
Giannou C. War Surgery, vol. 1. International Committee of the Red Cross, ICRC. May 2010, chapter 5, pp 95-125.
Hospenthal DF, Murray CK, Andersen RC et al. Executive summary: guidelines for the prevention of infections associated with combat-related injuries: 2011 update. Endorsed by the infectious diseases society of America and the surgical infection society. J Trauma. 2011;71:S202-209
Lin DL, Kirk KL, Murphy KP, et al., Evaluation of orthopaedic injuries in Operation Enduring Freedom. J Orthop Trauma. 2004;18(5):300-305.
Murray CK, Obremskey WT, Hsu JR et al. Prevention of infections associated with combat-related extremity injuries. J Trauma. 2011;71:S235-257
Nessen S, Lounsbury DE, Hetz SP. War surgery in Afghanistan and Iraq. Dept. of the Army: Borden Institute, 2008.
Pollak AN, Calhoun JH. Extremity war injuries: state of the art and future directions. J Am Acad Orthop Surg. 2006;14(10):S1-S213.
The view(s) expressed herein are those of the author(s) and do not reflect the official policy or position of Brooke Army Medical Center, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of the Army, Department of Defense or the U.S. Government.
Materials and support for The Disaster Preparedness Toolbox is provided by Lt Col. Ky Kobayashi, MD and Col. Benjamin Kam, MD.


.png){kind=link}
{kind=link}
{kind=link}
.png){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}