

- Discussion:
- spondylolysis refers to radiolucent defect of pars interarticularis;
- if defect is large, it is seen on nearly all x-rays of lumbar spine;
- if it is unilateral, as it is in 20 to 25 per cent of patients, or if it is not accompanied by spondylolisthesis, it is
subtle finding;
- if child is being followed for progression of spondylolisthesis, radiographic technique must be identical at each visit;
- lateral radiograph, made w/ patient standing, is preferred;
- in adults, degree of slip is not altered by the position of body, and radiographs that are made w/ patient recumbent are satisfactory;
- Olbique Views:
- dx will be missed in 20 % of young symptomatic patients if oblique radiographs are not made;
- Scotty-dog sign of Lachapele, w/ defect appearing as a collar around the dog's neck is seen;
- in pt who has acute injury, gap is narrow & has irregular edges, whereas in pt who has long-standing lesion, edges are smooth & rounded,
suggesting a pseudarthrosis;
- width of gap depends on amount of resorption of bone after frx & on degree of spondylolisthesis;
- example of normal view: 
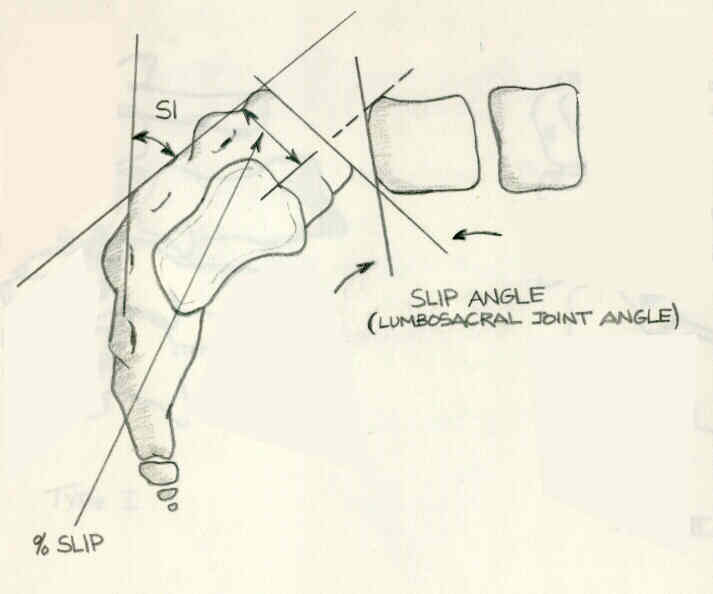
- Tangential Slipping:
- fifth lumbar vertebra slides forward on 1st sacral vertebra;
- top of sacrum is divided into four equal sections;
- slip in first quarter of the sacrum is grade I
- slip in last quarter is grade IV;
- grade V represents complete spondyloptosis;
- slip measurement:
- overlap of posterior part of cortex of L5 to posterior part of cortex of S1 is divided by maximum AP diameter of first sacral vertebra;
- Bone Scan: may be indicated w/ negative radiographic findings;
Radiographic evaluation of instability in spondylolisthesis.