

- Discussion:
- methods to enhance fixator stability;
- in the report by Minor T, et al, 37 femoral shaft fractures, in 33 pediatric patients, were treated with unilateral external fixation after reduction from 1992 through 1998 (ages from 4 to 14 years);
- average follow-up was 3 years, 9 months, with only five children lost to follow-up;
- average duration in fixator was 107 days;
- 36 of 37 fractures healed, and there was one delayed union;
- there was minimal angulation, and limb-length inequality was generally <1 cm; 72.7% had pin-tract infections.
- 8 (21.6%) patients refractured; four occurred in the four patients with bilateral femur fractures;
- children with bilateral femur fractures were at greatest risk.
- remember that the IT band may tether ex fix half pins, and therefore may a stellate perforation through the IT band to allow for knee flexion;
- ref: Outcomes of external fixation of pediatric femoral shaft fractures.
- external fixation vs flexible nails:
- in the study by Bar-on, et al (1997), flexible IM nails were compared to external fixation in a prospective study;
- consisted of a prospective study w/ 20 patients w/ age ranges from 5-15 years;
- in their study, time to full wt bearing, ROM, and return to school were all faster in the flexibile nail group;
- nails were inserted from the proximal end for more proximal fractures and from the distal end for more distal fractures;
- there were no cases of limb length inequality nor malunion in the nail group;
- ref: External fixation or flexible intramedullary nailing for femoral shaft fractures in children. A prospective, randomised trial


- Complications:
- up to 50% of patients may experience superficial pin tract infections, but most of these can be treated w/ PO antibiotics and will not require removal of the fixator;
- refracture may occur in 5-10% of patients (this may be prevented with dynamization of the external fixator within 2-4 weeks, depending on the stability of the fracture;
- fracture through a pin site is another complication which can occur if drill holes are not applied carefully;
- half pins should be less than 1/3 the diameter of the femur, inorder to lessen the chance of frx;
- in the report by Minor T, et al, 8 (21.6%) patients refractured; four occurred in the four patients with bilateral femur fractures;
- children with bilateral femur fractures were at greatest risk.
- ref: Outcomes of external fixation of pediatric femoral shaft fractures.
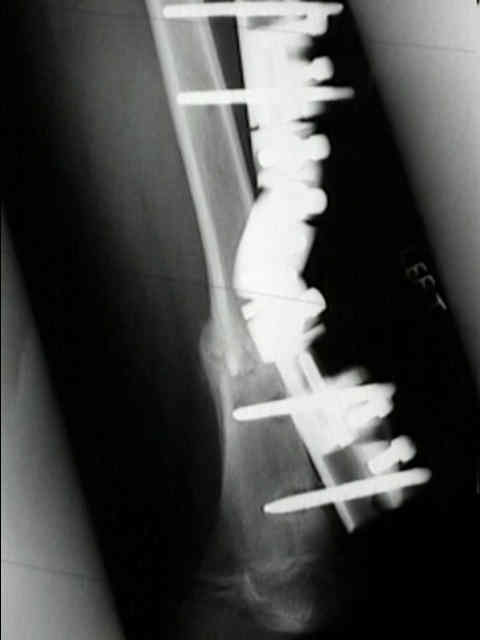
External fixation of pediatric femoral fractures.
Remodelling of angular deformity after femoral shaft fractures in children.
The use of external fixators in femur fractures in children.
Complex femur fractures in children: treatment with external fixation.
External fixation of femur fractures in children.
Radiological outcome after external fixation of 97 femoral shaft fractures in children.
Is external fixation in pediatric femoral fractures a risk factor for refracture?