


- Criteria for Instability: (see stable and unstable frx)
- loss > 50% of vertebral body height;
- angulation of thoracolumbar junction > 20 deg
- neurologic injury
- canal comprimise > 30 %
- spinal segment will fail w/ wt. bearing & early operative stabilization is advocated to restore sagittal
plane alignment;
- w/ residual canal comprimise is > 25-30% (in pt w/ incomplete neurological injury), secondary anterior retroperitoneal
decompression is perfomed;
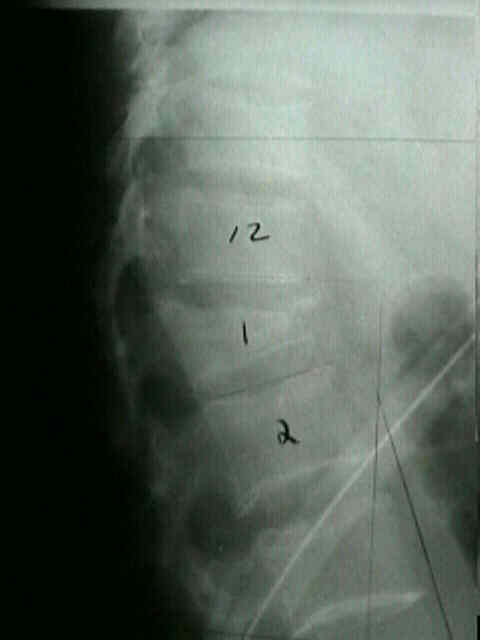
- Lateral View:
- in the study by Kuklo TR, et al (2001), the authors compared these methods for reliability and reproducibility of measuring
kyphosis on lateral radiographs;
- 50 lateral radiographs of thoracic and lumbar burst fractures were randomly selected and measured on two separate occasions
by three spine surgeons using five different measurement techniques;
- measuring from the superior endplate of the vertebral body one level above the injured vertebral body to the inferior endplate of
the vertebral body one level below) showed the best intraobserver and interobserver reliability overall;
- ref: Measurement of Thoracic and Lumbar Fracture Kyphosis Evaluation of Intraobserver, Interobserver, and Technique Variability.
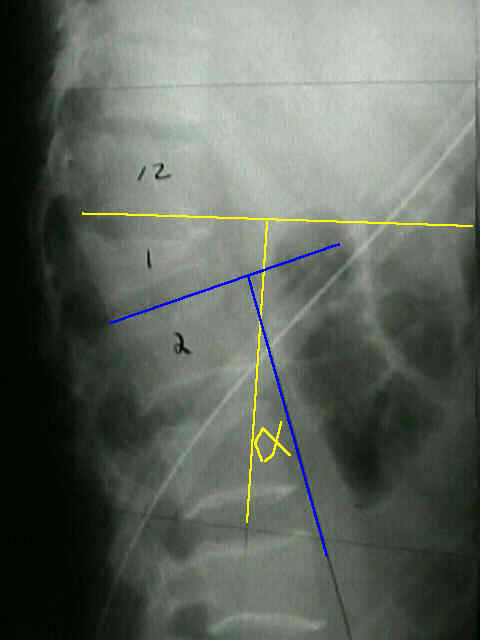
- assessment of stability using saggital index method:
- obtain lateral Cobb < (line extending from inferior end plate of involved vertebrae & line extending from inferior end plate of
superior vertebral body;
- SI = (lateral Cobb angle) - (baseline saggital curve);
- normal SI values:
- thoracic spine: 5 deg
- thoracolumbar spine: 0 deg (any amount of kyphosis in the thoracolumbar spine is abnormal);
- lumbar spine: negative 10 deg
- saggital index > 15 deg, may be indication for operative intervention
- it is also a deg which may require anterior vertebral fusion;
- willen wedge index:
- ratio of anterior vertebral body height to posterior vertebral body height;

 **
** 

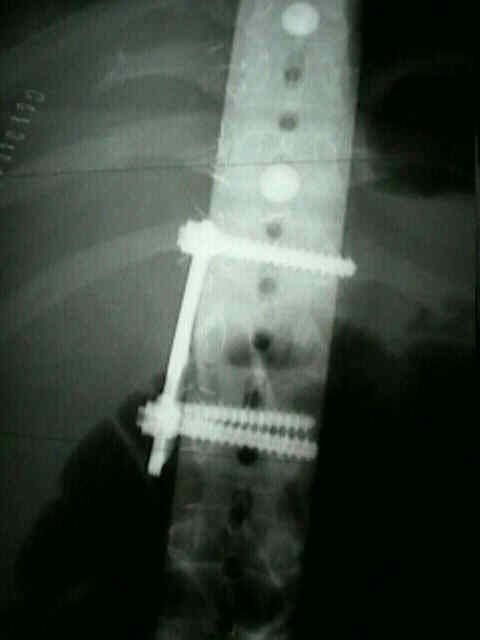
- AP View:
- Widening of Pedicles:
- there may be spreading of posterior elements, seen on the plain AP view of spine as a widening of interpedicular distance.
- w/ posterior element injury, neurologic injury is present in 50%;
- it is important to recognize that neural injury may be caused by neural element entrapment in laminar fractures.
- dural laceration should be suspected;
- Transverse Process Fractures:
- injuries are result of blunt trauma or violent contraction of the paraspinal musculature;
- when multiple frx are present as result of blunt trauma, esp when L-5 transverse process is frx, there is frequent assoc. w/
intra-abd. (particularly renal) injuries & pelvic disruption
Can burst fractures be predicted from plain radiographs
Sagittal index in management of thoracolumbar burst fractures.