

 - See: Midfoot/Forefoot Fractures
- See: Midfoot/Forefoot Fractures
- Discussion:
- involves frx at base of fifth metatarsal at metaphyseal-diaphyseal junction, which typically extends into the 4-5 intermetatarsal facet;
- Jones frx is located w/in 1.5 cm distal to tuberosity of 5th metatarsal & should not be confused w/ more common avulsion frx of 5 th metatarsal styloid;
- this fracture is usually proximal to the metatarsal cuboid joint;
- in addition, the acute Jones frx must be distinguished from the chronic Jones frx the later of which may represent a stress frx w/ poor prognosis for healing;
- hence, strictly speaking a Jones frx is an acute injury;
- Diff Dx:
- avulsion frx of base of 5th:
- this is the most common frx of the base of the 5th metatarsal;
- normal apophysis: 
- usually present between the ages of 9 to 14 years;
- apophyseal line runs parallel to shaft of metatarsal along its lateral-inferior margin of the tubercle;
- it does not extend proximally into the joint (unlike the fracture);
- os peroneum:
- ossicle in peroneus longus tendon where it is seen at the tip of the fifth metatarsal base;
- is seen in 15% of population;
- stress frx:
- these occur distal to the ligaments which firmly bind the 4th and 5th metatarsals together;
- these may be symptomatic before radiographic evidence of frx;
- w/ stress frx (indictating a chronic frx), an atheletic pt may benefit from ORIF;
- with closed treatment the rate of non union is 50%
- if non union has developed, with widening of frx line & sclerosis, cast mobilization is unlikely to be successful;
- consider bone-grafting & internal fixation w/ compression screw;
- Clinical Presentation:
- may present as acute lesion or may be seen in chronic phase, and either presentation has prolonged healing course, compared w/ frxs of other metatarsals;
- usually, there has been gradual onset of pain on outer side of foot, & only when pain interferes w/ walking does pt seek treatment;
- if several months have passed since the onset of symptoms, established non-union may already be present.
- radiographs show non-union and medullary sclerosis or even obliteration of the medullary canal;

- Radiographs:
- in addition to fracture location (which distinguishes avulsion from Jones frx), it is important to note characteristic features at the frx site;
- acute fractures should show sharp frx margins and no intramedullary sclerosis;
- delayed union will show persistent frx line in both cortices, periosteal callus (use hot lamp), and intra-medullary sclerosis;
- stress frx is revealed by a widened frx line and varying degrees of meduallary sclerosis;
- frx configuration in young adolescents:
- orientation of apophyseal line is parallel to shaft of metatarsal and it does not extend proximally into joint;
- frx lines tend to be oriented more transversely to the joint;
- Non Operative Treatment: (Acute Jones Frx)
- non operative treatment should be reserved only for acute frxs (in most cases);
- w/ a frx that is minimally displaced, is < 3 months old, and radiographs show frx w/o evidence of non-union (i.e., intra-medullary sclerosis and
a lucent fracture  line), non-operative treatment can be recommended;
line), non-operative treatment can be recommended;
- perhaps up to 2/3 of these fractures should heal;
- non-wt-bearing cast for 6-8 wks is necessary for healing;
- references:
- Fractures of the base of the fifth metatarsal distal to the tuberosity. Classification and guidelines for non-surgical and surgical management.
- Early Screw Fixation Versus Casting in the Treatment of Acute Jones Fractures.
- Shock Wave Therapy Compared with Intramedullary Screw Fixation for Nonunion of Proximal Fifth Metatarsal Metaphyseal-Diaphyseal Fractures
- The Association of a Varus Hindfoot and Fracture of the Fifth Metatarsal Metaphyseal-Diaphyseal Junction. The Jones Fracture
- Acute fractures to the proximal fifth metatarsal bone: Development of classification and treatment recommendations based on the current evidence.
 - Surgical Treatment: (Jones Frx);
- Surgical Treatment: (Jones Frx);
- patient is position in partial lateral position on bean bag;
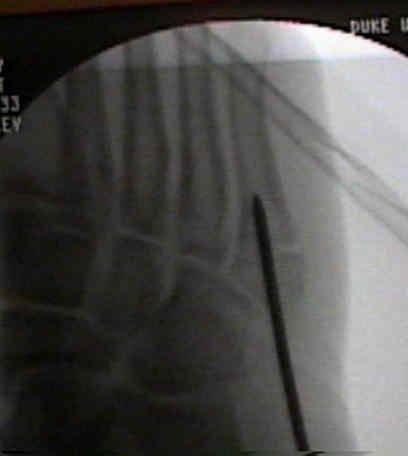
- flouroscopy:
- under flourscopic guidence, a K wire is inserted for determination of proper position and length;
- most common mistake is to direct the drill plantarly, rather than parallel w/ the shaft of metatarsal;
- second mistake is too position the guide wire using the oblique view;
- note that the metatarsal shaft is more narrow on the AP view, and it is possible for the pin to be centered on
the oblique view where as on AP view the pin is eccentrically positioned;
- incision:
- longitudinal incision is made over distal metatarsal;
- take care to avoid branches of the sural nerve which can course dorsally, and laterally over metatarsal;
- peroneus brevis is retracted inferiorly;
- insertion of this tendon may obscure the proper drill entry site;
- local bone graft:
- can be obtained from tuberosity and from bone bits from the drill; 
- implants:
- consider insertion of 4.5 cancellous bone screws, 4.5 mm cannulated screws (which are used in most cases) but
have available 5.5 cannulated screws and 6.5 mm cannulated screws;
- diameter should depend on width of the canal (let the screw tap help determine the best size);
- in either case, threads must cross the frx line;
- length is usually between 40-55 mm;
- consider countersinking the screw to avoid prominence of the screw head;
- in report by Kelly IP, et al, authors noted that failure is more likely when smaller diameter screws are used;
- experimental Jones fractures were created in 23 pairs of human cadaver fifth metatarsals, which were fixed using either 5.0 mm or 6.5 mm screws;
- frx stiffness and pull-out strengths were measured for either screw type and relationships with bone density and canal diameter were determined;
- poor thread purchase within the medullary canal was noted with the 5.0 mm screws, while excellent purchase was noted with 6.5 mm screws; 
- pull-out strength testing revealed significantly higher pullout strengths for the larger 6.5 mm screws;
- the authors conclude that larger diameter screws may be more appropriate for intramedullary screw fixation of Jones fractures;
- post op: patients will require protected postoperative wt bearing;
- ref: Intramedullary screw fixation of Jones fractures
- Outcomes:
- in the report by Larson CM, et al (2002), 15 patients (mean age, 21.7 years) underwent cannulated screw fixation of a Jones fracture;
- there were six treatment failures: four refractures and two symptomatic nonunions;
- mean time to full activity was 6.8 weeks for the patients with failure compared with 9 weeks for patients who did not have complications;
- although all patients were asymptomatic and radiographically progressing to union before return to full activity, only one of six patients with
failures had complete radiographic union, compared with six of seven patients with no complications;
- higher proportion of elite athletes (division I or professional level) among the failure group (83%) compared with those without complications (11%);
- return to full activity, especially among elite athletes, before complete radiographic union was predictive of failure
- ref: Intramedullary Screw Fixation of Jones Fractures. Analysis of Failure
Fractures and anatomical variations of the proximal portion of the fifth metatarsal.
The Jones' fracture in the nonathlete.
Jones fracture. Surgical versus nonsurgical treatment.
Jones' fractures and related fractures of the proximal fifth metatarsal.
Fractures of the fifth metatarsal. Analysis of a fracture registry.
Fractures of the base of the fifth metatarsal distal to the tuberosity: a review.
Outpatient percutaneous screw fixation of the acute Jones fracture.
Treatment of fractures of the fifth metatarsal: a prospective study.
Intramedullary screw fixation of Jones fractures.
Intramedullary screw fixation of the fifth metatarsal: an anatomic study and improved technique.
Closed intramedullary screw fixation for nonunion of fifth metatarsal Jones fracture
Likelihood of Surgery in Isolated Pediatric Fifth Metatarsal Fractures