

- See:
- ALIF with Revision Decompression and Reinstrumentation
- Anterior-Posterior Lumbar Interbody Fusion
- Posterior Lumbar Single-Level Decompression and Fusion with Instrumentation
- Anterior Arthrodesis of the Subaxial Cervical Spine:
- AAOS - Bulletin: A minute of malpractice
- Cage Fixation: (interbody fusion)
- provides excellent stabilization in flexion and lateral bending, but poor stabilization in extension and rotation;
- advantage: may offer fusion rates of over 90% and does not interfere with posterior musculature;
- disadvantage is that a decompression is not possible (if the anterior approach is utilized);
- complications may be higher when cage fixation is performed through a posterior approach;
- specifically this approach may cause chronic radiculopathy due to epineural fibrosis caused by the added epidural manipulation
which is required for this technique;
- another complication associated with a posterior approach is retropulsion of the cage back into the spinal canal causing neurological deficit;
- references:
Interbody cage stabilisation in the lumbar spine. Biomechanical evaluation of cage design, posterior instrumentation and bone density.
Interbody fusion cages in reconstructive operations on the spine.
- Pedicle Screw Fixation:
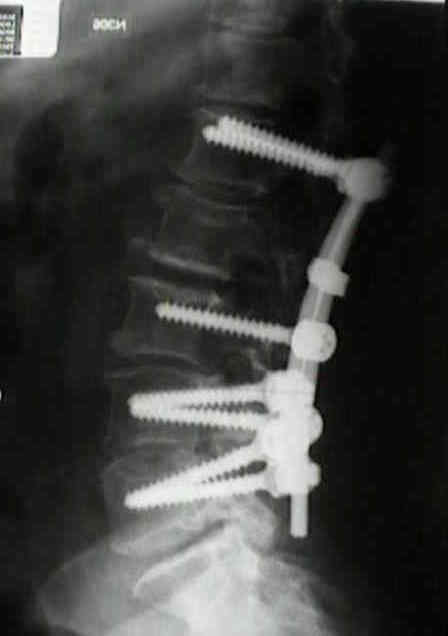
- pedicle screw fixation is generally felt to enhance spinal fusion by providing rigid fixation of spinal vertebrae;
- in the prospective study by France et al 1999, the authors did not find that pedicle screw instrumentation benefited
patients undergoing spinal fusion, except in patients with degenerative spondylolisthesis;
- patients with degenerative disc dz had 63% good to excellent results w/ instrumentation vs 73% w/o instrumentation;
- in those w/ degenerative spondylolisthesis, good to excellent results were found in 80% of patients w/
instrumentation vs 40% w/o instrumentation;
- S1 dorsal screw placement:
- in the anatomic study by Ebraheim, et al (2000), the authors determined the safe zone for S1 screw placement;
- using a starting point located inferlateral to the S1 superior facet, the authors recommend screw direction
30 to 40 deg lateral to avoid comprimising the lumbrosacral trunk and SI joint;
- insertion medial to this direction, might injure the L4 or L5 nerve roots;
- ref: - complications:
- nerve root irriation may be more common with medially placed screws;
- Castro, et al (1996), performed a study of 30 patients with 131
screws placed under flouroscopic control;
- CT images showed cortical penetration in 40% and medial wall penetration in 29%;
- deviation on CT of more than 6mm indicated a high risk of nerve root injury;
- references:
The lumbosacral nerves in relation to dorsal S1 screw placement and their locations on plain radiographs.
Accuracy of pedicle screw placement in lumbar vertebrae.
A randomized prospective study of posterolateral lumbar fusion. Outcomes with and without pedicle screw instrumentation.
Complications Associated with Pedicle Screws.
Segmental pedicle screw fixation or cross-links in multilevel lumbar constructs. A biomechanical analysis.
- Pseudo-arthrosis
- risk factors include: previous surgery, increased number of fusion levels;
- exam findings:
- worsening of preoperative symptoms;
- localized lumbar tenderness;
- diagnostic studies:
- radiographs: look for hardware failure;
- flexion / extension radiographs (look for abnormal translation);
- 4 mm of translation or more than 10 deg of angular motion between adjacent end plates (comparing
flexion and extension views);
- upto 3 mm of motion can be a normal finding;
- bone scan:
- increased uptake has little predictive value until one year after surgery;
- AP tomograms:
- best radiographic test for pseudoarthrosis;
- references:
- Assessment of pseudoarthrosis in pedicle screw fusion: A prospective study comparing plain radiographs, flexion-extension radiographs, CT scanning, and bone scintigraphy with operative findings.
- Failure of technetium bone scanning to detect pseudoarthroses in spinal fusion for scoliosis.
- A comparison of different methods used to diagnose pseudoarthrosis following posterior spinal fusion for scoliosis.
- surgery:
- allows best assessment of non-union
Early rod-sleeve stabilization of the injured thoracic and lumbar spine.
Interbody fusion and instrumentation.
Anterior lumbar fusion options. Technique and graft materials.
Indications for lumbar spine fusion in the adult.
Anterior fusion of the lumbar spine. End-result study with long-term follow-up.
Use of cortical cancellous allograft for posterior spinal fusion.
Treatment of symptomatic flatback after spinal fusion.
The syndrome of inappropriate antidiuretic-hormone secretion following spinal fusion.
Posterolateral lumbar and lumbosacral fusion with and without pedicle screw internal fixation.
Anatomic and technical considerations of pedicle screw fixation.


