

- See:
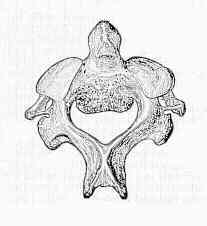
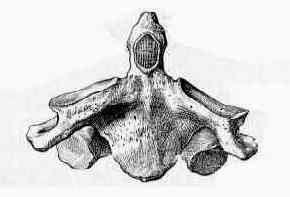
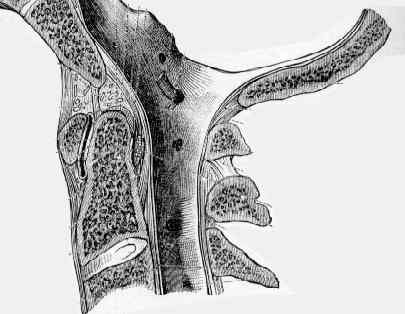
- Anatomy of C2
- Development of Dens
- Odontoid view:
- Pediatric Dens Frx:
- Discussion:
- odontoid fractures are the most common upper Cervical Spine fractures;
- remeber rule of thirds - cervical cord occupies a 1/3 of canal, dens occupies a 1/3, and the remaining 1/3 is empty;
- mechanism:
- flexion loading is the cause in the majority of patients, and results in anterior displacement of the dens;
- extension loading (forward fall onto forhead) occurs in a minority of patients, and results in posterior displacement of the dens;
- Normal Views: 


- Classification: (from Anderson LD, D'Alonzo RT (1974))
- Type I:
- this form of dens fracture is rare;
- oblique avulsion frx of tip of dens caused by an avulsion of alar ligament;
- type I frx is avulsion of alar lig off one side of tip of dens;
- alar ligaments connect the dens to the occiput.
- alar ligaments connect the dens to the occiput;
- evaluation should include dynamic lateral views to rule out anterior subluxation of C1;
- may be associated with occipitoatlantal dislocation (unstable injury);
- treat with a semirigid collar;
- cervical collar for symptomatic management is usually sufficient.
- ref: Fractures of the Odontoid Process of the Axis
- Type 2 Dens Frx:
- Type III:
- extends into the vertebral body of C2
- this frx allows the Atlas and the occiput to move as a unit, hence it is mechanically unstable - heals well w/ immobilization;
- any combination of angulation and translation can occur;
- cervical orthosis may be most appropriate in select pts w/ stable, impacted frxs, particularly elderly patients.
- frequent f/u is recommended for patients treated in this manner.
- healing in fully anatomic position is not likely w/o prolonged traction;
- most typical treatment is 12 weeks of immobilization w/ halovest, and majority of patients heal by bony union;
- anterior screw fixation:
- in the study by Henry et al, 81 patients with odontoid fractures underwent anterior screw fixation.
- 29 patients had type II fractures and 52 patients had type III fractures;
- 92% of patients achieved bony union at an avg of 14 weeks;
- two patients required seceondary posterior fusion;
- full range of motion was restored in 43 patients;
- ref: Fixation of odontoid fractures by an anterior screw.
- Associated Injury:
- Atlas Frx: (see: Jefferenson Frx)
- halovest until the C-1 arch is healed, then a posterior C-1 & C-2 arthrodesis if the dens has not healed;
- it is prudent to obtain a CT scan of the C-spine, in all patients w/ a dens frx, esp if C1-C2 fusion is being considered;
- Transverse Ligament Rupture:
- may occur in 10% of patients w/ type II dens fracture;
- MRI is used to make the diagnosis;
- non operative treatment would be expected to result in atlantoaxial instability;
- Pharangeal Injury:
- ref:
Transverse atlantal ligament disruption associated with odontoid fractures.
Posterior atlanto-occipital dislocation with fractures of the atlas and odontoid process.
Odontoid Fracture Associated with a Pharyngeal Tear. A Case Report.
C2 Vertebral Fractures in the Medicare Population
Fractures of the dens. A multicenter study.
Avascular necrosis of the proximal end of the dens. A complication of halo-pelvic distraction.
Odontoid fractures, with special reference to the elderly patient.
Anterior stabilization for acute fractures and non-unions of the dens.
Injuries of the atlas and axis. A follow-up study of 85 axis and 10 atlas fractures.