

- Indications for Closed Reduction and Fixation:
- indications for closed reduction and fixation:
- physiologically young patient: age < 65, working patient, good bone stock;
- demented elderly patient that requires total care;
- adequate closed reduction w/ no frx comminution or femoral neck defects;
- patient should be aware that with an inadequate closed reduction, then an open reduction or hemiarthroplasty will be required;
- Radiographs: - accetable reduction parameters
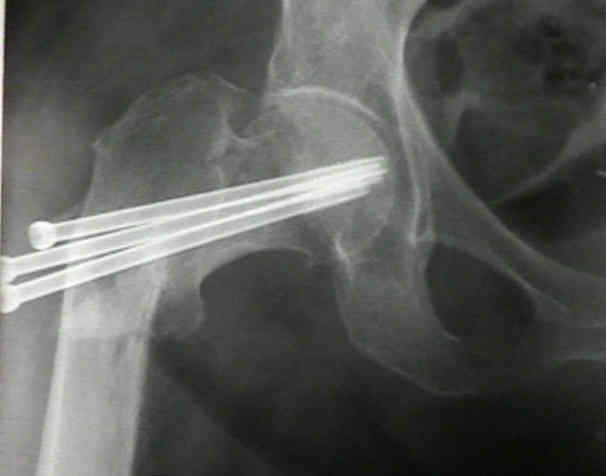
- Screw Insertion Technique:
- technique of closed reduction
- positioning:
- supine position on the fracture table:
- this is the optimal position for fracture fixation, assuming that a satisfactory reduction is obtained;
- advantage is that it is easy to directed the guide pins into the femoral neck and head, since an AP and surgical lateral
flourscopic view can be obtained w/o having to move the patient's hip;
- disadvantage is that if reduction slips, it can be difficult to re-reduce the hip while the hip is in extended position
on fracture table;
- lateral position:
- main advantage is that the fracture table is not required and that hip can be re-reduced if the initial reduction is lost;
- main disadvantage is that frx reduction may slip as the hip is flexed and externally rotated (for the frog leg lateral view);
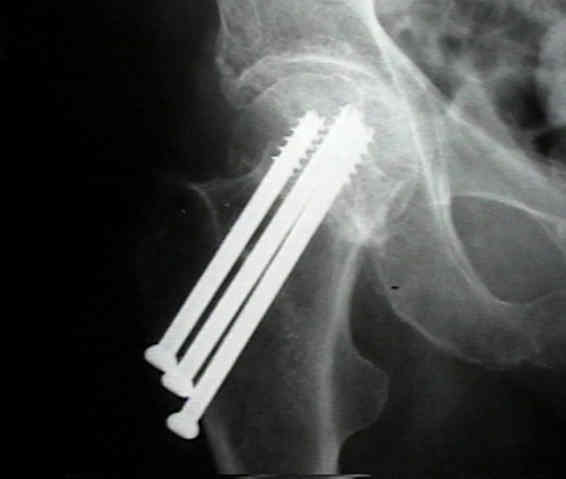
- configuration and number of screws
- guide pin insertion point and angle of insertion
- Using a cannulated screw as a drill guide and sleeve: for multiple-screw fixation for intracapsular femoral neck fracture.
- Minimal Effect of Implant Position on Failure Rates in Femoral Neck Fractures: Commentary on an article by Anne Marie Nyholm, MD, et al.: "Osteosynthesis with Parallel Implants in the Treatment of Femoral Neck Fractures. Minimal Effect of Implant Position on Risk of Reoperation".
- Osteosynthesis with Parallel Implants in the Treatment of Femoral Neck Fractures: Minimal Effect of Implant Position on Risk of Reoperation.
- Is the Cranial and Posterior Screw of the "Inverted Triangle" Configuration for Femoral Neck Fractures Safe?
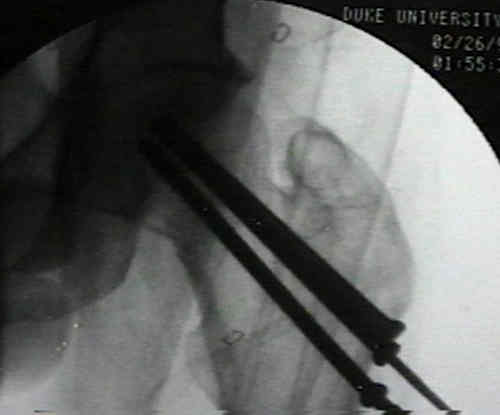
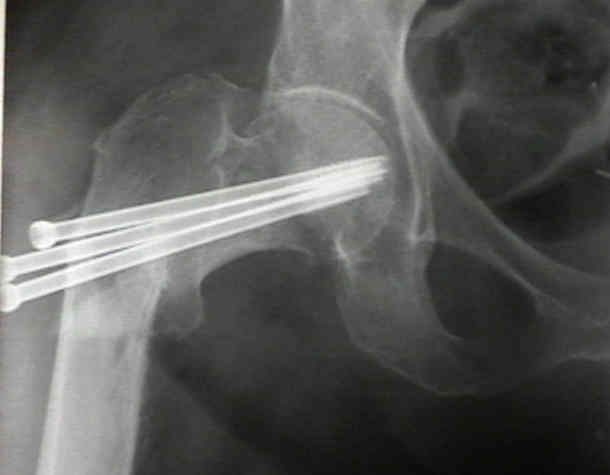
- depth of guide pin placement:
- under flouroscopy, guide-pin is drilled into place along medial cortex of femoral neck & into head to within 5 mm of
subchondral bone;
- cannulated drill is then placed over each pin and drilling carried out to depth of 5 to 10 mm short of the tip of the pin to keep
guide wire from coming out;
- length of screws to be implanted is determined by direct measurement of guide pins, which have been inserted just shy of
subchondral bone;
- cautions: if screw and guide pins need to be repositioned due to mismeasurement, replace the guide pin using the blunt end so
as to avoid joint penetration;
- references:
- Articular penetration is more likely in Garden-I fractures of the hip.
- Subchondral screw fixation for femoral neck fractures.
- Prevention of unrecognized joint penetration during internal fixation of hip fractures: a geometric model based on Steinmetz Solid.
- [Femoral neck fractures: position of the implant, unrecognized articular penetration and its consequences]
- [Predictive criterions of unrecognized articular effraction after internal fixation of femoral neck fractures].
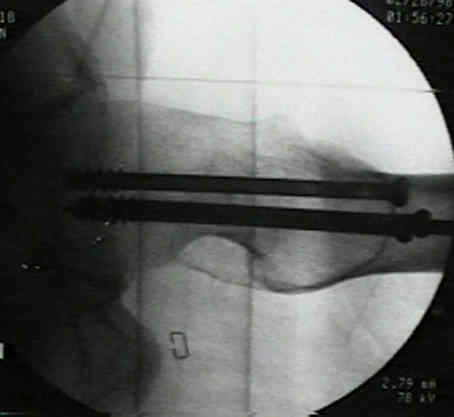
- screw selection and insertion: (see insertion of pins for hip frx)
- in very dense bone, a tap should be utilized into femoral head, but generally is only necessary in lateral cortex;
- in most systems there are two screw-thread lengths available: short and medium;
- essential that all screw threads are past frx site (inorder to achieve compression), and therefore short threaded screws will often
be required;
- screws are then inserted and retightened after any traction that has been placed on the limb has been released;
- inferior screw is placed first, followed by the superior screws;
- guide wire is removed after screw has passed across fracture to prevent advancing the guide wire into the hip joint;
- screws are tightened simultaneously, to apply uniform compression across frx & to avoid tipping of femoral head into varus
angulation;
- reference:
- Short versus long thread cannulated cancellous screws for intracapsular hip fractures: a randomised trial of 432 patients.
- Use of fully threaded cannulated screws decreases femoral neck shortening after fixation of femoral neck fractures.
- washers: role in maximizing compresssion;
- The value of washers in internal fixation of femoral neck fractures with cancellous screws: A biomechanical evaluation.
- impaction of frx:
- w/ dense bone, impaction of frx can be performed after traction is released by applying mallet blows to a broad bone tamp
placed on lateral surface of the proximal femur adjacent to screws;
- following such impaction, the screws should be retightened in hopes of maintaining interfragmentary compression;
- anterior capsulotomy
- some surgeons feel that these patients require emergent reduction and pinning along with capsulotomy (to avoid hematoma
and increase in intra-articular pressure);
- Intraosseous pO2 in femoral neck fracture. Restoration of blood flow after aspiration of hemarthrosis in undisplaced fractures.



- Post Operative Care:
- forces acting on the hip joint
- as noted by Koval KJ, et al (1998), elderly patients who are allowed to bear wt as tolerated, will voluntarily limit loading of
the injured limb;
- references:
- Postoperative weight-bearing after a fracture of the femoral neck or an intertrochanteric fracture.
- Complications:
- avascular necrosis:
- Asnis SE and Wanek-Sgaglione L (1994), patients who develop AVN following hip frxs may continue to maintain high level
of function;
- loss of fixation and non-union:
- references:
- Complications following young femoral neck fractures.
- Failure Patterns of Femoral Neck Fracture Fixation in Young Patients
- subtrochanteric fracture:
- if guide pins are inserted into the lateral cortex at a point below the lesser trochanter a stress riser will be created, risking frx;
- holes at this location have been associated with 20 % prevalence of subtrochanteric frx;
- references:
Intracapsular Fractures of the Femoral Neck. Results of Cannulated Screw Fixation.
Subtrochanteric fracture after cannulated screw fixation of femoral neck fractures: a report of four cases.



Subcapital fractures of the femur. A prospective review.
Intracapsular fractures of the femoral neck. Results of cannulated screw fixation.
Femoral neck fractures in skeletally mature patients, fifty years old or less.