- See: Bone Graft Menu
- PreOp Planning:
- if patient has undergone previous bone graft harvests, consider CT scan to determine amount of remaining bone left in the crest;
- in the report by Ahlmann E, et al, the authors investigated whether
there was less morbidity with an anterior versus posterior approach;
- medical records of 88 consecutive patients who had undergone a total of 108 iliac crest bone-grafting procedures for the
treatment of chronic osteomyelitis from 1991 to 1998 were retrospectively reviewed.
- 66 anterior and 42 posterior bone-graft harvest sites were evaluated at a minimum of two years after the operation;
- major complication was associated with 8% (five) of the sixty-six anterior sites and 2% (one) of the 42 posterior sites;
- rates of minor complications were 15% (ten) and 0%, respectively;
- rates of both minor complications (p = 0.006) and all complications (p = 0.004) were significantly higher after the anterior
harvest procedures than they were after the posterior procedures.
- postoperative pain at the donor site was significantly more severe (p = 0.0016) and of significantly greater duration (p =
0.0017) after the anterior harvests;
- ref: Comparison of Anterior and Posterior Iliac Crest Bone Grafts in Terms of Harvest-Site Morbidity and Functional Outcomes
- Posterior Crest Harvest
- Anterior Crest Cancellous Graft Harvest:
- this technique may provide 10-15 cc of cancellous bone, and will cause the patient minimal symptoms;
- make a small, 4-5 cm incision just below the anterior iliac wing;
- once down to the periosteum, elevate a small, 2x2 cm area on top of the crest;
- note that further periosteal stripping will result in increased postoperative pain;
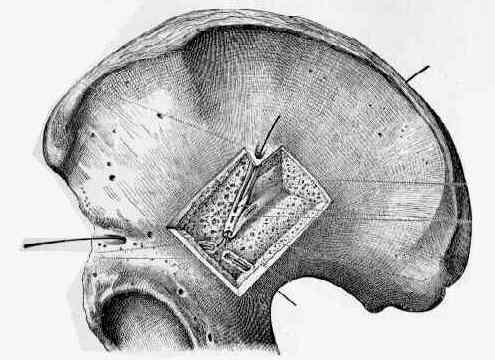
- use a rongeur to remove a small window, 1.5 x 1.5 cm on top of the crest;
- carefully use a currett to extract cancellous bone from between the inner and outer tables;
- infuse marcaine or similar long acting anesthetic;
- Anterior Crest: Corticocancellous Graft Harvest
- bicortical harvest:
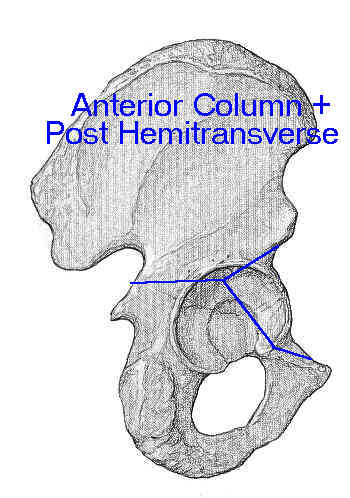
- bicortical grafts should be harvested at least 2 cm posterior to the ASIS, inorder to avoid fracture;
- anterior crest harvest - inner table
- Donor Site Morbidity After Anterior Iliac Bone Graft Harvesting.
- anterior crest harvest - outer table:
- disadvantages:
- hematoma formation is more with anterior harvest than posterior harvest (since compression of posterior harvest site occurs
in supine position);
- hematoma is prevent by placing 1 or 2 drains along the cancellous graft harvest site;
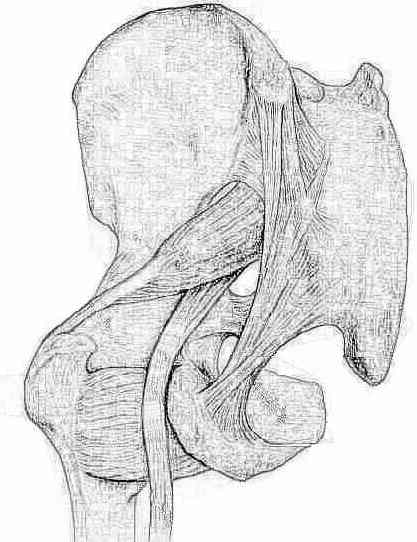
- gluteal lurch gait:
- occurs from excessive stripping of the gluteus medius from the outer table;
- ASIS avulsion: prevented by keeping the harvest 2 cm posterior to the ASIS;
- Post Operative Care:
- as noted by Sasso, et al (1998), there was no apparent advantage or disadvantage to use of drains for iliac crest donor sites;
- Postoperative drains at the donor sites of iliac-crest bone grafts. A prospective, randomized study of morbidity at the donor site in patients who had a traumatic injury of the spine.
Harvesting autogenous iliac bone grafts. A review of complications and techniques.
Fracture at the iliac bone graft harvest site after fusion of the spine.
Bone graft harvest site as a determinant of iliac crest strength.
Fracture at the iliac bone graft harvest site after fusion of the spine.
A technique for obtaining bone graft.
Donor-site morbidity after harvesting rib and iliac bone.
A new technique for obtaining iliac bone grafts.
Procurement of Bone Graft from the Iliac Crest. An Operative Approach with Decreased Morbidity.
Cloward technique for obtaining iliac crest bone graft in hand surgery.
The proximal tibia metaphysis: a reliable donor site for bone grafting?