

- See:
- FDP Avulsion
- FDP Lacerations
- tendon pull thru technique
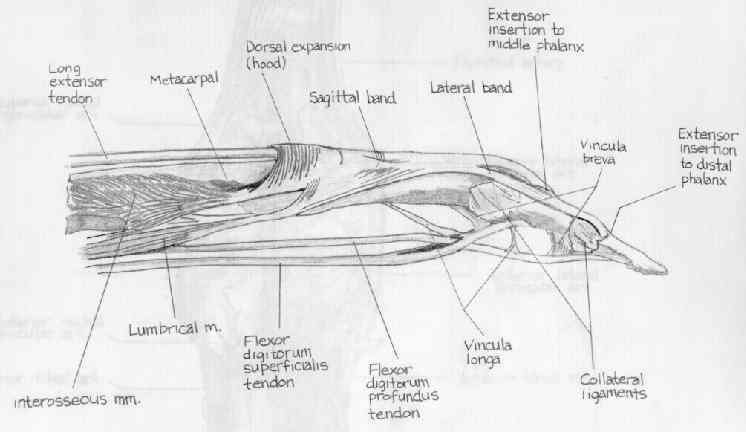
- Anatomy:
- in zone 1, FDP has emerged from between & beneath decussating FDS and travels to its insertion in the distal phalanx;
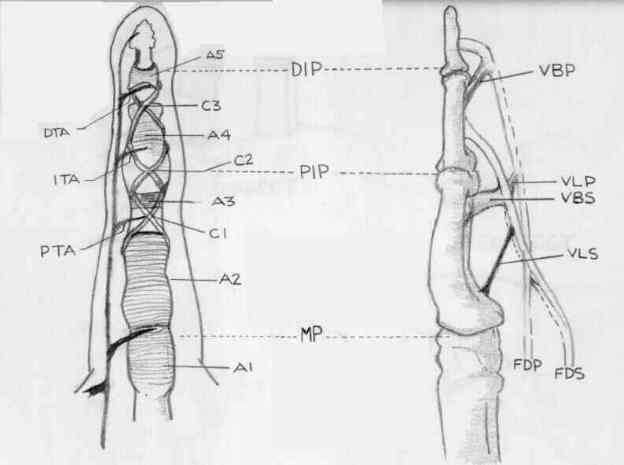
- zone 1 contains: A4, C3, and A5 pulley;
- A4 pulley must be preserved, otherwise the majority of active PIP flexion will be lost;
- Injury Pattern:
- most injuries are due to lacerations, but traumatic rupture from phalangeal attachment may occur; (see: FDP avulsion:)
- Exam:
- when FDP is divided in zone 1, there is loss of active flexion of distal phalanx, as well as a hyperextension instability of distal IP joint;
- this results in instability, esp when these injuries are in index & middle figners, because w/ unstable pinch, pts tend to drop things easily;
- if tendon has retracted into the proximal finger or palm after rupture or laceration, pt will be unable to actively move distal phalanx;
- dx is made by asking him to flex distal phalanx & watching level of ability to flex digit;
- if proximal end of flexor profundus becomes caught at the level of sublimis chiasm, it may affect the range of activemovement at PIP joint;
- in this area repair may be delayed upto 3 weeks;
- if tendon is held by vinculum, some active flexion may be possible;
- if tendon has retracted into the palm, it is difficult to reattach stump if injury is beyond 10 days old;
- Treatment Options for Zone 1 Lacerations:
- treatment may consist of direct repair or tendon advancement;
- for tendon lacerations w/in 1 cm of insertion, profundus tendon can be advanced and attached to the distal phalanx;
- for clean, fresh, sharp lacerations more than 1.5 cm away from the insertion, primary tenorrhaphy is the treatment of choice;
- Surgical Technique:
- wound edges are extended, debrided, and irrigated;
- proximal tendon edge of tendon is identified;
- typically the proximal tendon edge can be found just proximal to the PIP joint and is restrained by the viniculum;
- it may be necessary to open either the C2 or C1 pulleys for tendon retrieval;
- distal tendon edge
- if digit was flexed at time of injury, then distal tendon stump will be short;
- determine how far the laceration is to the insertion of the tendon;
- tendon exposure and opposition:
- w/ an especially short distal tendon stump, open the C3-A5 sheath;
- through the appropriate proximal window (C2 or C1), a core suture is placed;
- this core suture is then passed underneath the A4 pulley, and subsequently the proximal tendon stump is passed proximally;
- the tendon is temporarily anchored by passing a 25 gauge needle thru the annular pulley;
- tendon repair:
- if laceration is more than 1 cm from insertion, perform primary repair using standard repair techniques;
- tendon advancement:
- see tendon pull thru technique
-----------------------------------------------------------------------------