

- Two Incision Exposure:
- prior to open exposure, a markedly displaced frx should be reduced and held in place w/ K wires;
- 6-7 cm linear incision beginning 2 cm proximal to Lisfranc joint & extending distally over first intermetatarsal space;
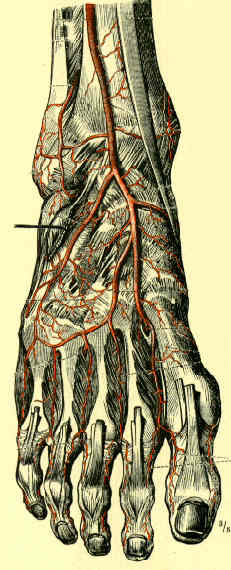
- avoid damage to dorsalis pedis artery and deep peroneal nerve;
- if 3rd metatarsal is dislocated, make 2nd dorsal linear incision between the third and fourth metatarsals;
- 1st and 2nd joint capsules are opened thru dorsal incisions, which allows exposure to the joint surfaces;
- alterantive incisions:
- dorsal incision over 2nd metatarsal (for fixation of 1st to 3rd rays);
- lateral incision is made in 4th interspace;
- One Incision Exposure:
- longitudinal incision centered over naivular and medial side of 3rd metatarsal;
- dissect along the lateral border of the EHL, which should then reveal dorsalis pedis artery and deep peroneal nerve;
- follow the neurovascular bundle to the 1-2 interspace;
- cauterized the perforating artery between the 1-2 interspace;
- the EHL and N/V bundle are retracted laterally, to expose the 1-2 interspace, and in contrast, the EHL and neurovascular bundle is retracted medially to expose the 3-4 articulation;
- exposure 1-2 interspace, inspect articulations, remove bony fragments;
- in some cases, there will be instability between the cuneiforms, which will require modification of the screw insertion strategy