

- See: Technique of Free Tendon Grafting
- Discussion:
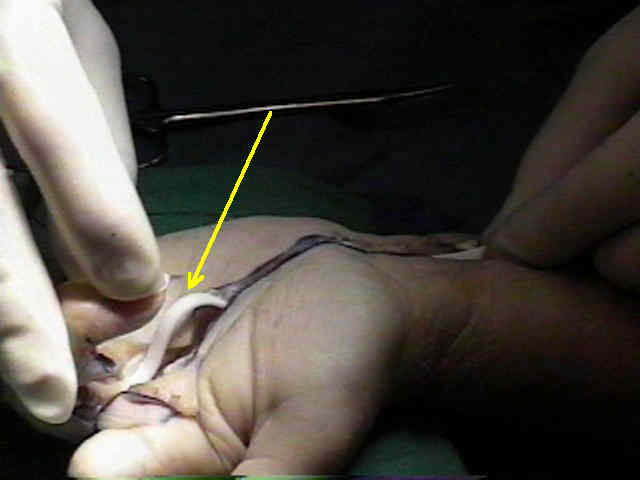
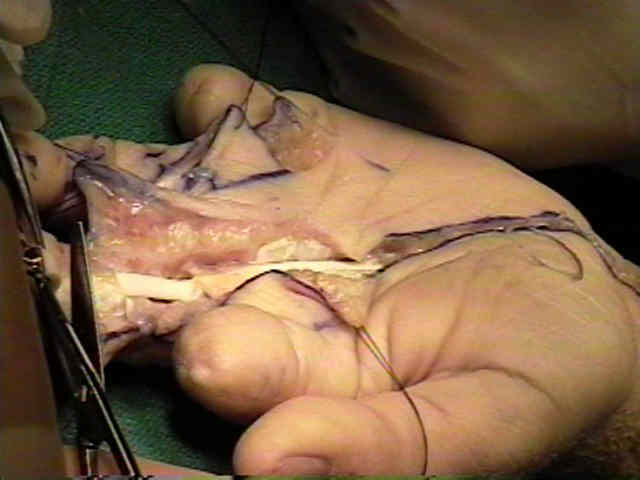
- prosthetic graft serves as temporary spacer around which a pseudotendon sheath forms, & provides a healthy bed in which to place tendon autograft;
- pulleys can be reconstructed at time of insertion of prosthesis
- two prostheses available are passive and active tendon implants;
- typically prosthesis remains in place for at least 3 months, after which time secondary tendon grafting can be performed;
- indications:
- loss of pulley system
- extensive scaring w/ in tendon bed
- dirty graft bed
- presence of stiff joints: ROM must be regained after silicone elastomer rod is inserted;
- Types of Implants:
- passive implant:
- is attached to remaining flexor tendon (pull thru technique) or bone (1.5 mm or 2.0 mm screws) and is left unattached proximally for a distance 4-6 cm proximal to the carpal tunnel and deep to the FDS;
- passive motion will promote the development of pseudo-sheath;
- implant gliding motion is obtained by active finger extension and passive flexion;
- proximal end of the rod must be left free proximally, otherwise the rod can rupture;
- pulley reconstruction should be performed at the same time as insertion of passive implant;
- once the rod has been passed thru each pulley, taken the digit thru a full range of motion;
- determine correct rod size:
- usually 4 mm rod is appropriate (Wright Medical Technology, Arlington, TN)
- if rods are seen to bowstring, then the pulleys are too loose;
- if rods are seen to buckle, then the pulleys are either too tight, or they are bunching up at the proximal end;
- the later is addressed by cutting the rod short and by ensuring that there is a deep enough pocket to allow rod motion;

- in order to avoid, silicone synovitis, avoid rod contact w/ foreign bodies, such as the powder found on newly opened surgical glooves;
- surgical glooves should be rinsed free of gloove powder prior to contact with the silicone rod;
- acitve rod:
- is similar to passive rod but has a Darcon silicone loop or cords proximally to attach to the proximal motor (which is usually FDP);
- these rods are not design to function as permanent implant;
- ruptures are known to occur at the distal attachment site;
- best method of attachement involves suture pull thru technique;
- Pearls
- leave the rod out until all of the pulleys have been reconstructed;
- next secure the rod distally (sutures or screws), and subsequently pass the rod
from distal to proximal using a tendon passer;
- it will be necessary to make a 2 cm transverse incision in the mid-forearm in order to insert the tendon passer from proximal to distal (inorder to pull the rod distally);
- ensure that the rod has been passed thru each reconstructed pulleys (i.e., ensure that none of the pulleys have been missed)
- Complications:
- silicone synovitis:
- patient may note redness, swelling, and pain;
- once infection has been ruled out, immbolize the hand;
- in most cases, rod removal will not be necessary
Development of a reconstituted collagen tendon prosthesis. A preliminary implantation study.