

- Anatomy:
- radiographic teardrop:
- true floor of acetabulum corresponds to the radiographic teardrop;
- teardrop lies in the inferomedial portion of the acetabulum, just above the obturator foramen;
- the lateral and medial lips corresponds to the external and internal acetabular walls, respectively;
- the medial wall is a relatively constant radiographic finding and is not significantly distorted by small degress of rotation (unlike the
ilioischial line - Kohler's line);
- the tear drop may appear less prominent on obturator oblique views in which case;
- the tear drop gives an accurate assessment of how much medialization is necessary to have the acetabular component rest on the
true acetabular floor;
- ilioischial line: (Kohler's line)
- as pointed out by Goodman et al (1988), the ilioischial line does not consistently represent true acetabular floor;
- anatomically the superior ilioischial line is formed by the broad cortical surface of the siciatic notch (which lies posterior to the
acetabular floor), and the inferior ilioischial line is formed by the cortical surface of the anteiror ischium;
- hence, anatomically this line does not correspond to the acetabular floor;
- on straight AP radiographs, the ilioischial line will overlie the acetabular floor, but with any amount of rotation, this relationship will diverge;
- indeed, the entire medial wall may be reamed out, without disrupting Kohler's line;
- The acetabular teardrop and its relevance to acetabular migration.
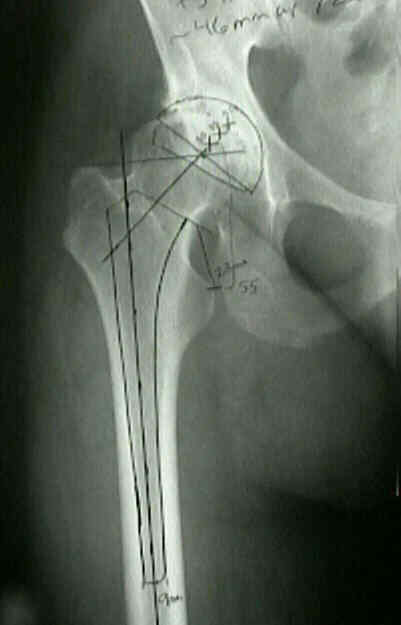
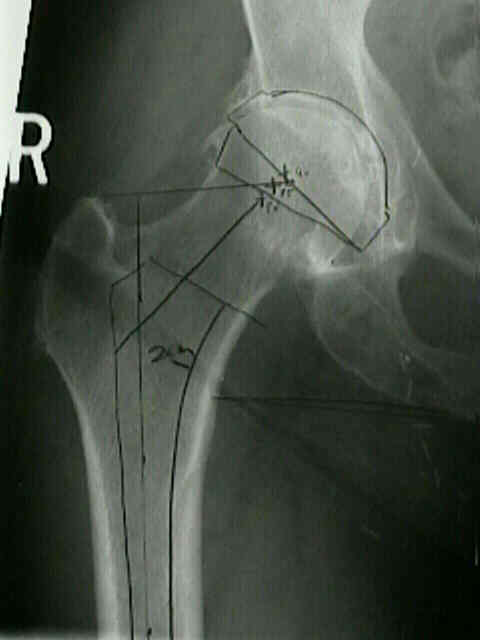
- Templating:
- AP of pelvis:
- mark center of of acetabular component: this will correspond to the new center of rotation;
- AP of pelvis to determine whether the bone is OK for fixation of the acetabular cup, to estimate how much reaming will be necessary, &
to determine whether a bone graft will be required to support cup & whether protrussion or osteophyte formation may make dislocation of the hip difficult;
- place the acetabular overlay templates on film and select size that matches contour of patient's acetabulum, w/o removing excessive subchondral bone;
- medial position of acetabular template is at teardrop & the inferior margin is at level of obturator foramen;
- in making a template for acetabular component, medial aspect of the prosthetic acetabulum should be just lateral to lateral edge of the tear drop;
- inferior part of cup should be at level of bottom of tear drop;
- superior position is marked by the true superior edge of the acetabulum (as oppossed to super osteophytes which have grown out laterally over
the superior acetabular margin;
- determination of acetabular anteversion: (see Adult Anteversion)
- acetabular retroversion is present when posterior acetabular margin ends in a more medial position than the anterior margin in relation
to the superior aspect of the acetabular rim;
- anterior and posterior margins of the acetabulum should be approximately 1.5 centimeters apart as measured from the center of the femoral
head in a plane that is vertical to the anterior aspect of the acetabular rim;
- decrease in this distance suggests a decrease in acetabular anteversion;
- increase in this distance suggests an increase in acetabular anteversion;


- lateral of pelvis: (Standing):
- need to determine status of posterior column, esp in revsion surgery;
- template the femur on the lateral view in a similar manner to asses if implant determined on AP can be inserted w/o excessive bone
removal;
- McCollum's Line:
- standinng lateral x-ray of pelvis centered over greater trochanter.
- line is drawn between the sciatic notch and ASIS and its angle from the horizontal is measured;
- this line may range from 0 degrees to +40 degrees (nl 20 deg);
- w/ a lordotic spine, expect a smaller angle and therefore the acetabular component needs to be flexed more than usual;
- Technical Considerations:
- lateral offset:
- in osteoarthritis acetabulum is often overgrown by osteophytes that push the femoral head laterally, superiorly, and posteriorly;
- in order to re-establish optimal hip mechanics, the hip center must be placed medially, inferiorly, and anteriorly;
- note that medialization down to the true inner table which decreases the offset more than 1 cm
will weaken the abductors, will increase joint reaction forces, and may lead to THR instability;
- this decrease in offset can be managed appropriately by using an increased offset femoral stem;
- always know ahead of time whether the implant you are using has the option of an increased offset femoral stem in addition to
knowing the modularity lengthening options of the femoral head;
- references:
- The offset problem in total hip arthroplasty. Steinberg B, Harris WH. Contemp Orthop. 1992;24:556-562.
- protrusio:
- dysplasia
- center edge angle
- to determine the adequacy of the superior lip of the acetabulum, draw line from the lateral aspect of the acetabulum down to inferior
aspect of the teardrop, and measure the angle between this line and a horizontal line;
- if angle is > 45 deg, acetabular dysplasia is probably a problem, and superior bone grafting may be necessary;
- bone grafts for acetabular reconstruction:
- assess availability of bone stock for acetabular reconstruction;
- to determine the adequacy of the superior lip of the acetabulum, draw a line from the lateral aspect of the acetabulum down to the
inferior aspect of the teardrop;
- measure the angle between this line and a horizontal line;
- if this angle is > 45 deg, acetabular dysplasia is probably a problem, and superior bone grafting may be necessary;
- bone erosion:
- if center of acetabulum of affected hip will be placed more proximal than that of non affected hip, as a result of superolateral bone loss,
surgeon needs to compensate for this change to maintain equal leg length;
- this can be done in one of two ways:
- by making a more proximal femoral neck cut and seating femoral component less deeply into the proximal femur, of by using a longer femoral neck;
- conversion of hemiarthroplasty to THR
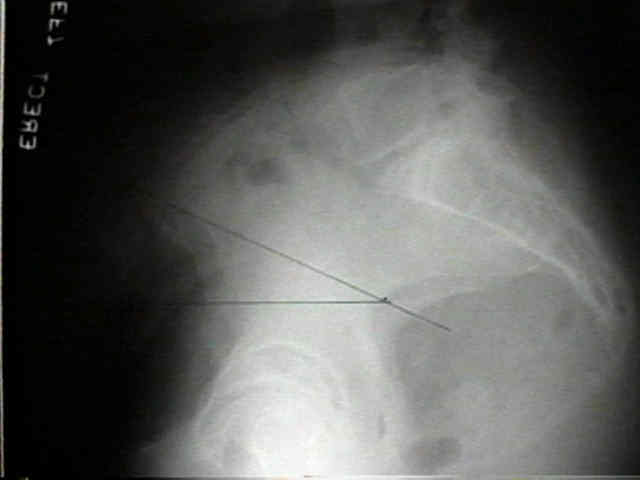
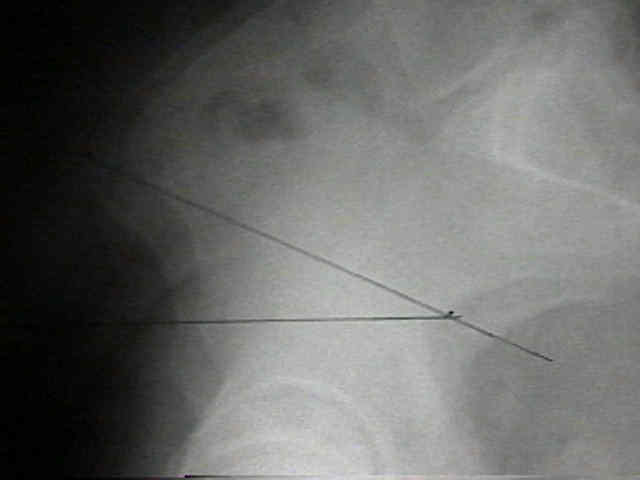
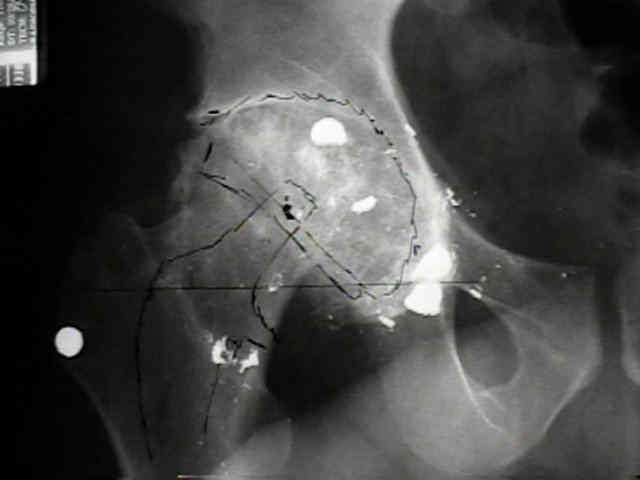
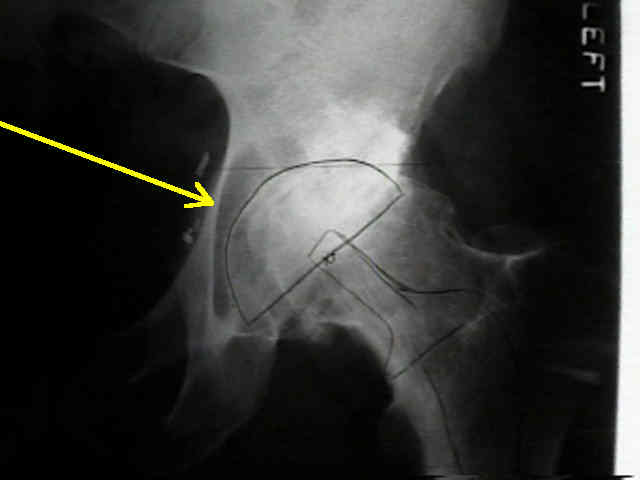
- Case Example:
- 35-year-old male w/ near anklyosed hip following a GSW to the hip;
- preoperative films appeared to indicate that little or no medialization was necessary;
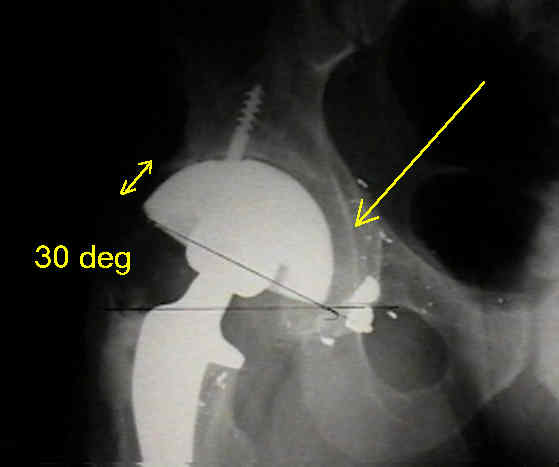
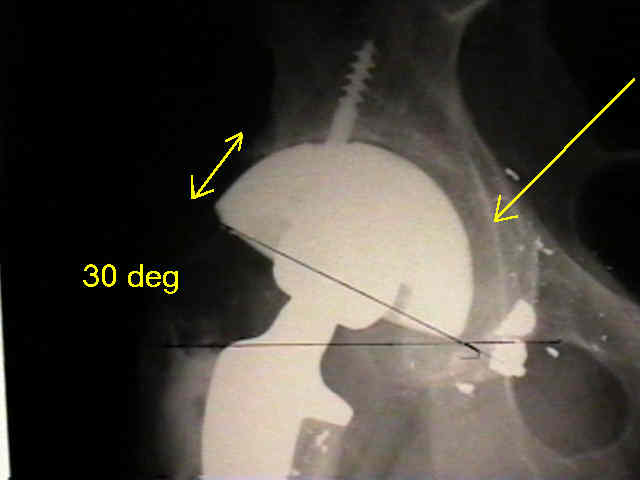
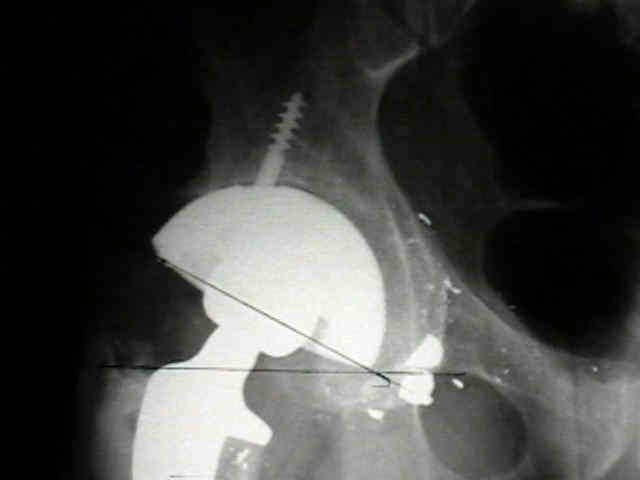
- postoperative films, however, indicate that the cup was lateralized (hence, reaming was inadequate);
- in retrospect, the radiographs which are rotated externally (like an iliac oblique) tend to falsely minimize the necessary amount of
medialization where as radiographs which are rotated internally (like an obturator oblique), tend to over-estimate the necessary
amount of medialization




- Acetabular Cyst:
The acetabular tear drop and its relevance to acetabular migration.
Reconstruction of the hip. A mathematical approach to determine optimum geometric relationships.
The use of preoperative computed tomography scanning in total hip arthroplasty.
The value of preoperative planning for total hip arthroplasty.