- See: Autograft Discussion
- PreOp Planning:
- if patient has undergone previous bone graft harvests, consider CT scan to determine amount of remaining bone left in the crest;
- Technique:
- ensure that appropriately sized self retaining retractors are available;
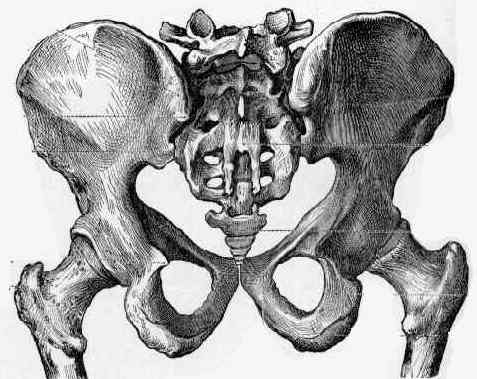
- straight longitudinal incision is made over posterior superior iliac spine;
- transverse oblique incisions are to be avoided because of the superior clunial nerves which usually cross the crest 8 cm lateral to the PSIS;
- an alternative incision is an oblique incision from proximal-medial to distal-lateral, which is parallel to the clunial nerves, and which is perpendicular to the posterior crest;
- as noted by Colterjohn, et al (1997), this approach will improve superficial incision tenderness, but will not affect deep tenderness;
- incise thru the subcutaneous tissues, and identify the fascia of glutues maxiumus which blends in with the fascia of the external oblique;
- incise the maximus subperiosteally off of its origin;
- using a key elevator, subperiosteally elevate the crest along the superior and lateral surfaces;
- avoid incising thru or stripping the posterior ligamentous complex of the SI joint, since this may lead to SI joint instability;
- a Taylor retractor can be inserted at this time;
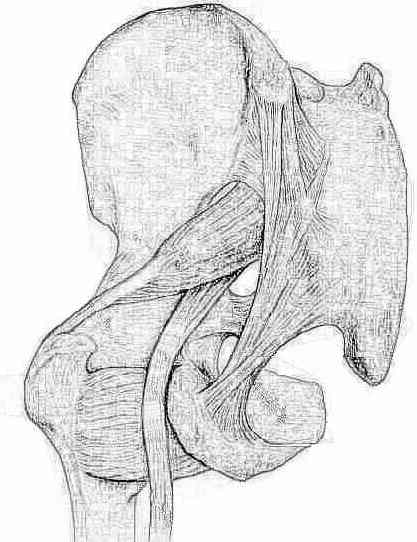
- inferiorly, the greater sciatic notch should be palpated prior to instrumenting in this area;
- injury to the superior gluteal artery is a potential complication of posterior crest harvest;
- in some cases this can be managed by exposing and ligating the vessels, with bone removal from the notch;
- in cases of superior gluteal vessel injury, also look for possible injury to the adjacent ureters;
- bone graft can be harvested to within 1 cm of the notch;
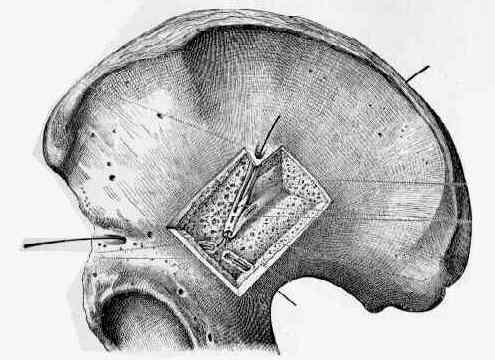
- using an osteotome, a trapezoidal outline is marked thru the cortical surface of the outer table;
- begin outlining the graft, along the farside (anterior) aspect of the graft, since this is the first area to be covered up by bleeding;
- smaller longitudinal cortical strips can also be outlined at this time;
- curved gouges are then used to remove longitudinal cancellous strips;
- this is continued down to the level of the inner table;
- currettes are used to remove additional cancellous bone from the superior and medial rim of the crest;
- hazards:
- superior clunial nerves arise from the L1-3 dorsal rami and extend over the superior buttocks and posterior iliac crest;
- these nerves cross the crest 8 cm lateral to the midline;
Procurement of Bone Graft from the Iliac Crest. An Operative Approach with Decreased Morbidity.
- Post Operative Care:
- as noted by Sasso, et al (1998), there was no apparent advantage or disadvantage to use of drains for iliac crest donor sites;
- references:
- Postoperative drains at the donor sites of iliac crest bone grafts. A prospective randomized study of morbidity at the donor site in patients who had a traumatic injury of the spine.
Harvesting autogenous iliac bone grafts. A review of complications and techniques.
Fracture at the iliac bone graft harvest site after fusion of the spine.
Fracture at the iliac bone graft harvest site after fusion of the spine.
Bone graft harvest site as a determinant of iliac crest strength.
A technique for obtaining bone graft.
Donor-site morbidity after harvesting rib and iliac bone.
A new technique for obtaining iliac bone grafts.
Procurement of Bone Graft from the Iliac Crest. An Operative Approach with Decreased Morbidity.
Cloward technique for obtaining iliac crest bone graft in hand surgery.