

- Discussion:
- flexion contractures of PIP joint are more difficult to correct;
- flexion deformities of PIP joint may be caused by contracture of a diseased central cord (which is an extension of palmar pre-tendinous cord);
- PIP join contracture may be presaged by development of firm, fixed nodule at proximal phalanx level;
- flexion deformities may remain or recurr due to:
- pericapsular fibrosis;
- shortening of palmar plate checkrein;
- accessory collateral ligaments;
- divided at their attachment to palmar plate;
- scarring of the FDS to the proximal phalanx or volar plate (requires tenolysis)
- contracture of flexor tendon sheath;
- correction can sometimes be obtained by a transverse division of tendon sheath just distal to the A2 pulley (over C1 pulley);
- Surgical Considerations:
- consider Agee Digit Widget;
- its better to accept mild contracture (upto 20 deg) than to release palmar plate from neck of proximal phalanx;
- remember that contracted PIP joint that is functional (participates in grip, ect) is more beneficial than an extended but stiff PIP joint;
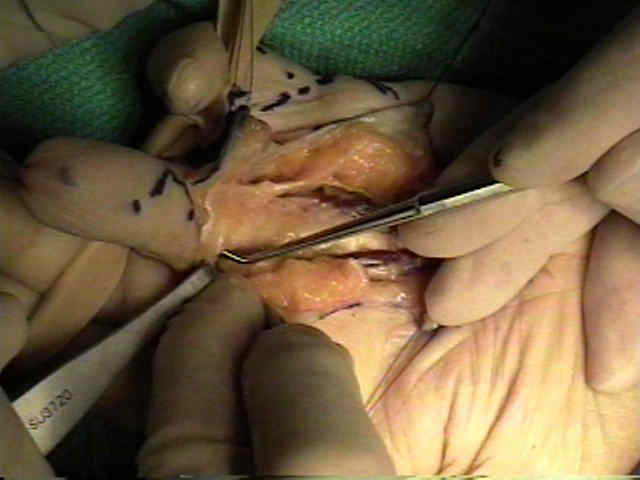
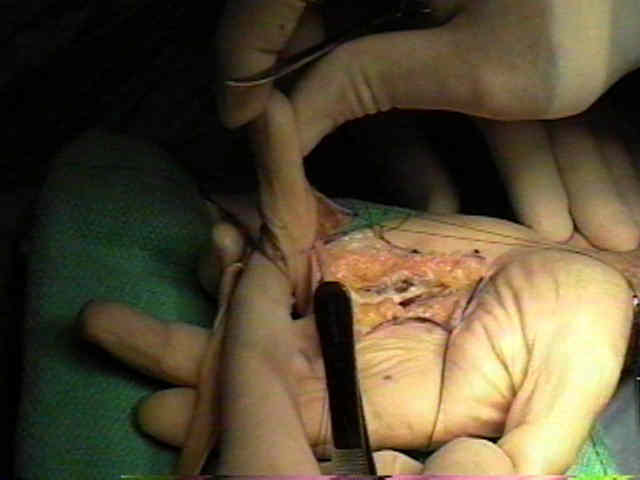
- excessive dissection around the PIP joint risks excessive post-op scarring and stiffness;
- scarring is especially likely to occur when the joint is entered;
- often, a mild flexion contracture of the PIP joint will improve w/ PT, after fascial excision;
- hence, in most cases the dissection should be limited to the spiral cords, C3 tendon sheath pulley, and checkreins;
- in the finger, Cleland's ligaments are dorsal to the neurovascular bundle and are less involved as compared to Greysonn's ligaments;
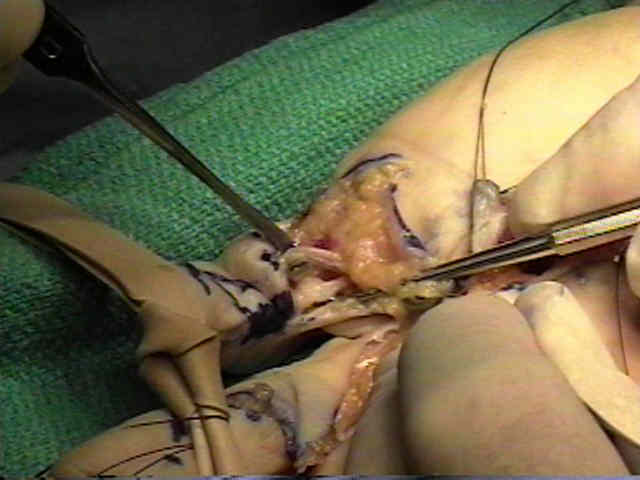
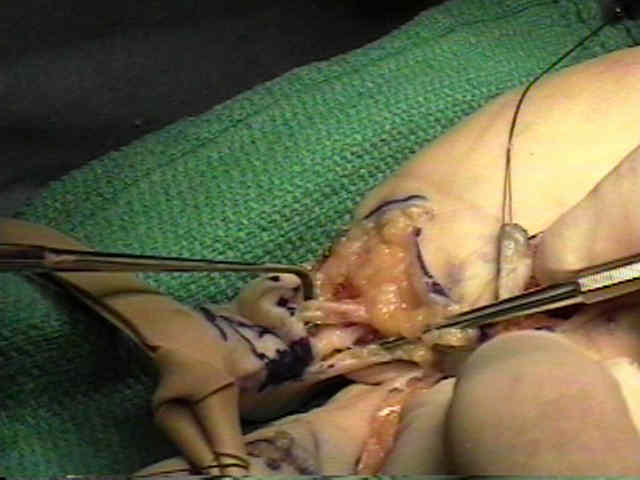
- Checkreins:
- normally the volar plate is not attached to the proximal phalanx, but in Dupuytren's contracture, fibrous checkreins develop between the proximal
corners of the volar plate and the fibro-osseous sheath;
- should be released, sparing digital arterial branches to vincular system running immediately dorsal to them;
- they pass 3 mm proximal to the proximal edge of the volar plate;
- care is also taken to avoid entering the PIP joint, since this may lead to more scarring;
- ref: Checkrein resection for flexion contracture of the middle joint. HK Watson, TR Light, TR Johnson. J. Hand Surg. Vol 4: 1979. p 67.
- K wires:
- w/ contracture more than 80 deg, consider insertion of K wires to hold the joint extended;
- take care that forced extension, does not lead to excessive wound tension, or flap ischemia;
- K wires are thought to increase the possibility of infection;
- Wound Closure:
- in some cases, it may be necessary to apply a FTSG to the skin defect;
- Salvage:
- salvage options for severe PIP contractures include fusion, skeletal shortening, interpositional arthroplasty, and amputation;
- Post Op Dressing:
- w/ chronic PIP contracture, too much extension may lead to digital vascular compromise;
- if the PIP joint has been entered, then earlier and more aggressive hand therapy may be required
Severe contractures of the proximal interphalangeal joint in Dupuytren's disease: results of a prospective trial of operative correction and dynamic extension splinting.