

- Discussion:

- not all patellar fractures are amenable to ORIF;
- in most cases of patellar frx, one large frag of patella can be preserved;
- most often the distal pole is comminuted, whereas superior pole is intact,however, as a principle, the larger
fragment is preserved;
- goal is to minimize any abrupt change in the articular surface to avoid DJD;
- patients should expect a signifacant loss of extensor strength postoperatively;
- Technique:
- its helpful to preserve as much of length of patellar ligament or quadriceps tendon as possible;
- its important to try to maintain the length of the remaining ligament or tendon without excessive shortening;
- otherwise, the pt may develop a patella baja;
- its important to leave a small fragment of bone attached into patellar tendon;
- starting near articular surface, drill 2 holes in a proximal direction;
- it is controversial as to whether to attach the patellar tendon (and its bony remnant) to the
anterior or posterior surface of the remnant patellar fragment;
- placement near the anterior border of the patella (away from the articular edge) may optimize
the remaining patellofemoral contact area and patellofemoral function;
- this may be the preferred technique;
- placement near near articular surface allows minimal step-off between the tendon and remaining
intact cartilage, tends to avoid tilting of the patellar remnant following repair;
(hence, avoid tendon attachment to the anterior patellar surface);
- reference: Effects of partial patellectomy and reattachment of the patellar tendon on patellofemoral contact areas and pressures.
- Suture Technique: 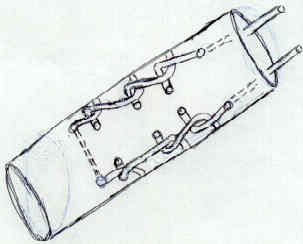
- similar to patella tendon repair;
- Adjunctive Reenforcement Techniques:
- serves as an adjunt to suture tendon repair and protects tendon repair as the patient is started on early motion;
- 1.5 mm drill hole is made in the tibial tubercle, 1 cm deep to the tubercle;
- suture technique:
- either No 5 Ethibond suture or Merserline tape is passed thru the tibial tubercle, is crossed in front of the patellar remnant and is then
passed deep thru the quadriceps tendon;
- wiring technique:
- 18 gauge wire is passed through transverse drill holes made through the patellar fragment and thru the tibial tubercle;
- the knee is flexed to 90 deg prior to tightening the sutures;
- wire is tightened to the point that tension is taken off the tendon, but not to the point that the patella is brought distally;
- patient should be forewarned that the wires frequently break and will typically require removal;
- Complications:
- suture pull out:
- partial patellectomy with suture of patellaar ligament to patella may fail if the sutures pull out;
- look for proximal migration of upper patellar pole on radiography or by absence of palpable quad tendon repair to inferior pole fragment;
- there will be absence or weakness of quadriceps function;
- inability to palpate the patellar ligament or detection of a gap between ligament & pole fragment supports diagnosis;
- Patellectomy:
- similar exposure as for partial patellectomy;
- saw blade (followed by osteotome) is used to split the patella longitudinally down the middle;
- the remanat patellar fragments are then enucleated w/o disrupting the overlying soft tissues;
- the defect is then repaired side to side in a "pants over vest fashion;"
- ensure that the knee can flex to 90 deg without difficulty;
- ensure that there is not lateral subluxation of the tendon (in which case, retinacular release is required)
Partial patellectomy for patellar fracture: tension band wiring and early mobilization.
Treatment of patellar fractures by partial patellectomy.
Results of treatment of displaced patellar fractures by partial patellectomy.
Knee function after patellectomy and cruciform repair of the extensor mechanism.
Knee function after patellectomy. A 12- to 48-year follow-up.
Effect of patellectomy on the function of the quadriceps and hamstrings.
The effect of patellectomy on knee function.