

 - Surgical Approaches:
- Surgical Approaches:- if operative treatment has been selected, it is essential that a near anatomic reduction be obtained;
- malunion may lead to reduction is subtalar motion and eventual arthrosis;
- its essential to avoid varus and dorsal angulation;
- the area of the talus that has the most bone density the lateral aspect of its head and neck;
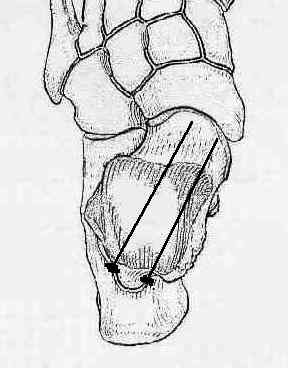
- typically, two parallel screws are inserted, one partially threaded and one fully threaded;
- excessive lag screw compression is avoided, especially if there is excessive medial or dorsal comminution since
this will deform fracture reduction;
- Posterolateral
- recommended approach for screw insertion but does not allow frx visualization;
- dissects between the achilles tendon and peroneal tendons;
- allows posterolateral to anteromedial screw placement, which is perpendicular to the fracture line;
- disadvantage: does not allow direct view of fracture reduction;
- Anteromedial:
- advantage: gives excellent exposure allows surgeon to adress medial sided comminution;
- disadvantage: disruption of medial blood supply to talus
- fixation of talar neck fractures on the medial side is difficult because of the narrow limits of screw placement but medial exposure
is recommended when there is concomitant medial malleolar frx (thru the frx site);
- medial approach is also required when the tibialis posterior has become interposed;
- made medial to the tibialis anterior over the neck of the talus;
- medial osteotomy: (see AO foundation discussion)
- can be performed at the same time, gives wide exposure neck and body;
- medial malleolar step-cut osteotomy allows for for reliable placement of the osteotomy and secure anatomic reduction;
- medial malleolus is predrilled with 2 holes to allow for anatomic reduction at end of the procedure;
- oscillating saw is used to make transverse osteotomy 1 cm proximal to the ankle to a level even with the axilla of the mortise;
- small osteotome is used to complete step-cut osteotomy from anterior to posterior, being careful not to enter medial malleolus;
- release the posterior tibial tendon along the posterior aspect inorder to mobilize the medial malleolus;
- anterior joint capsule is released to the level of the deltoid ligament;
- care is taken not to disrupt the deltoid ligament;
- fixation:
- screw placement is from anterolateral to posteromedial into dense talar bone;
- this reduces the tendency for the fracture to collapse into varus malalignment;
- references:
- Direction of the oblique medial malleolar osteotomy for exposure of the talus
- Step cut osteotomy of the medial malleolus for exposure of the medial ankle joint space.
- Medial Malleolar Osteotomy for Exposure of Complex Talar Body Fractures
- Oblique medial malleolar osteotomy for the management of talar dome lesions.
- Anterolateral
- similar to Ollier for Sinus Tarsi / lateral neck
- advantage: preserves blood supply to talus;
- disadvantage / cautions:
- relatively poor expsure for internal fixation;
- be sure that the talar body can be reduced before using this approach, since the tibialis posterior tibial tendon can block the
reduction (and access to the tendon is not possible with this approach);
- Implants:
- 6.5 mm cancellous bone screws or large cannulated screws as lag screws for talus neck fractures;
- 4.5 cortex screws or 4.5 mm cannulated screws as lag screws (neck frx in smaller bones)
- 3.5 mm cortex screws or 3.5 mm cannulated screws as lag screws (posterior body or neck fracture);
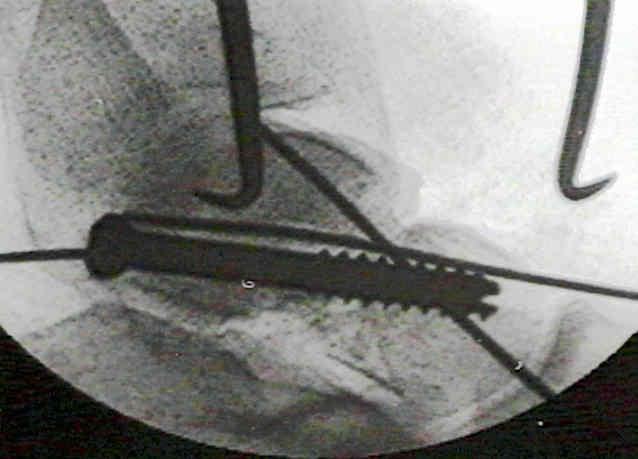
- anatomical reduction, closed or open, & provisional fixation w/ K wires
- insertion of 6.5 mm cancellous bone screw as lag screw from posterior direction (neck fractures);
- 4.5 mm drill bit is used to drill a gliding hole for the shaft in dense bone of the talus;
- 7.0 mm cannulated screw may be used as an alternative;
- K wire is inserted parallel to prevent rotation;
- insertion of 3.5 mm cortex screws or 4.0 mm cancellous screws as lag screws, from the medial side in complex frxs
Treatment of Comminuted Talar Neck Fractures with Use of Minifragment Plating.
Fractures of the talar neck: A mechanical study of fixation.
Talar neck fractures: Anatomic considerations for posterior screw application.
Medial malleolar osteotomy for exposure of complex talar body fractures.
Oblique medial malleolar osteotomy for the management of talar dome lesions.