- See:
- Distal Radius Frx Menu
- External Fixators for Distal Radius Frx
- Intra-Articular Fractures of the Distal Radius
- Unstable Distal Radius Frx
- Radiographs:
- scapholunate dissociation
- Technique:




- first perform closed reduction under flouro;
- if an assistant is not available, then the reduction must be held either w/ Chinese finger traps or a temporary external fixator;
- w/ excessive dorsal frx tilt, consider placing a K wire in a dorsal to plantar direction to help tease the frx into a normal palmar slope;
- consider using two or three crosed 0.062 in smooth K wires;
- radial styloid frx:
- the radial styloid frx is first stabilized to the diaphysis of the radius;
- generally is held w/ 2-3 0.045 (or 0.062) K wires inserted obliquely from distal to proximal, with the proximal wire tip embeded into the radial cortex,
- the starting point is located on the dorsal aspect of the radial styloid fragment, which helps avoid the radial artery;
- care must be taken to avoid the branches of the radial sensory nerve, by making a small incision and spreading w/ a clamp;
- a 14-gauge needle can be used as a soft tissue protector for a 0.045 K wire;
- 0.062 pins offer increased rigidity as compared to smaller sized pins;
- die punch fragment:
- following fixation of the radial styloid fragment, the remaining depressed articular fragments are elevated and reduced;
- reduction is facilitated w/ traction, direct pressure, or with use of a small incision and application of pointed reduction clamps;
- if reduction can not be performed closed, then a limited open reduction can be performed;
- wires can be inserted transverse across the subchondral portion of the distal radial articlular surface, either through the ulna and across the RU joint, or directed transversely thru the radial cortex to lie just under the subchondral surface;
- metaphyseal comminution:
- w/ high energy frxs or w/ metaphyseal comminution, consider combination of external fixation and bone grafting inorder to prevent late collapse of the articular reduction;




- Specific Techniques:
- Naidu Technique: (Naidu, et al (1997))
- two radial styloid pins along with a pin placed from the ulnar corner of the radius provides most biomechical stability;
- this was more stable than 2 radial styloid pins;
- Percutaneous pinning of distal radius fractures: a biomechanical study.
- Clancy Technique: (ref)
- two pins are inserted into the distal radius w/o involving ulna;
- one pin enters into the radial styloid (between the 1st and 2nd extensor compartments) and is driven toward the ulna;
- the 2nd pin is inserted along the lateral (ulnar) aspect of the distal radius between the 4th and 5th extensor compartments;
- the dorsal radial cutaneal nerves may be palpated prior to pin insertion;
- this technique has been criticized as not providing adequate stability, unless a long arm cast is applied;
- Case Examples:











- this 40-year-old patient underwent application of a external fixator prior to insertion of pins;


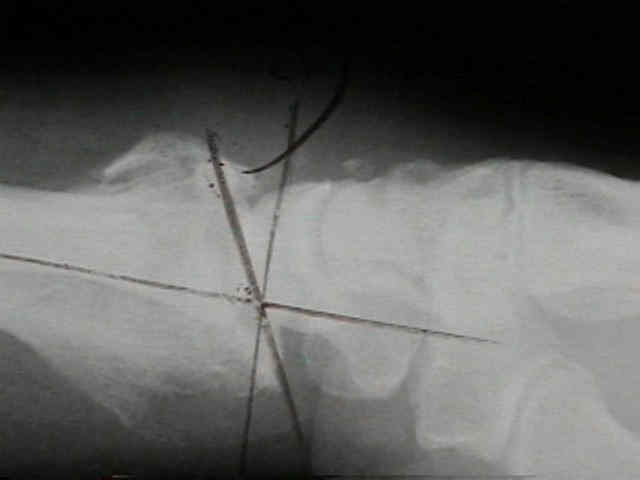








- note that prior to pin insertion, the external fixator was distracted to help maintain the reduction, but at the end of the case, the distraction was released and the reduction was rechecked w/ flouro;
- it is essential that the MP joints achieve full flexion at the end of the case, as overdistraction can lead to MP join clawing
Complications of distal radial fractures: pins and plaster treatment.
Percutaneous and limited open reduction of the articular surface of the distal radius.
Treatment of comminuted distal radius fractures with pins and plaster.
Percutaneous pinning of distal radius fractures: a biomechanical study.