
John E. Cunningham
INTRODUCTION
Pseudarthrosis, or non-union, is an all too common and expensive complication of spinal fusion surgery, with the cost per QALY (quality-adjusted life year) gained estimated to be about US$118,945.1 Rate estimates vary greatly between studies utilizing different surgical techniques and patient populations.2
Pseudarthrosis is usually defined as failure of bony union between two vertebrae within 12 months after surgery.3 Until solid bony fusion is achieved, the surgeon should not consider that their patient has reached a surgical endpoint, regardless of the initial indication for the fusion surgery.
Prevention of pseudarthrosis can be difficult, as can diagnosis and treatment. Part of the difficulty of prevention may be the risk factors of the patient that are often non-modifiable in the short term. Surgeons are encouraged to take note of these risk factors and modify their surgical treatment to ameliorate those risks as best they can. Occasionally, this may include delaying or even cancelling surgical intervention if the risk of pseudarthrosis and the resultant poor outcome outweighs any foreseen benefit of surgery.
The presentation of pseudarthrosis most often includes pain, which is usually central in nature and the onset of which may be many months following the operation. Investigation and diagnosis most commonly involves fine-cut CT scanning, and consideration of concomitant infection should always be included. Treatment most often involves revision surgery employing a multitude of techniques.
RISK FACTORS
Patient factors play a significant role with regards to pseudarthrosis risk. Smoking is one of the better studied risk factors.4,5 Brown et al., performed a randomized study of 100 patients undergoing two-level uninstrumented fusion from L4 to the sacrum.6 The non-smokers had a pseudarthrosis rate of 8%, whereas regular smokers had a rate five times higher, at 40%. A more recent study examined the impact of smoking in the presence of pedicle screw instrumentation, but without interbody devices.7 For single-level fusions they found no difference in fusion rates, but for two-level fusions, pseudarthrosis was three times higher (29% vs. 11%).
Other patient factors that influence union rate are those that should not come as a surprise to an orthopaedic surgeon, as they are similar to those for general non-unions. These include age, the use of steroids and NSAIDS, diabetes, malnutrition and prior surgery.8,9 Perioperative radiation decreases fusion rates as well,10 which needs to be taken into account when treating patients with tumors.
From a surgical point of view, the number of levels increases the risk of pseudarthrosis, as does the use of non-rigid fixation.9,11 Instrumentation of any kind increases the fusion rate over non-instrumented fusions.12 In order of fusion rates, circumferential fusion location gives the highest (interbody as well as posterolateral), followed by posterior interbody, anterior interbody and then posterolateral.11 There is evidence that titanium interbody devices fuse faster and more often than those made of PEEK.13-15
Pedicle Subtraction Osteotomy
The operation of pedicle subtraction osteotomy (PSO) is being performed in increasing numbers both due to our greater appreciation of sagittal malalignment as well as our aging population.16 One of the major complications is of pseudarthrosis, occurring in about 10% of patients.17 The pseudarthrosis most often occurs at the level of the osteotomy, and risk factors include performing the operation for the management of a pre-existing pseudarthrosis, preoperative radiation, the presence of a neurological or inflammatory disorder, and the lack of an interbody fusion directly above the osteotomy. This last observation is supported by cadaveric studies.18 It appears that interbody cages improve fusion rates by increasing the rigidity of the structure. It is also for this reason that the authors elect to add a third rod to PSO constructs, from a level above to a level below the osteotomy site using side-to-side connectors and a chrome-cobalt rod, similar to the technique described by Hyun et al.19
Spinal Deformity Surgery
In one study of deformity operations that included the sacrum, the pseudarthrosis rate was found to be 24%.20 All pseudarthroses were detected before four years after surgery at an average of 27 months, and either occurred at the thoracolumbar junction or at the lumbosacral junction. The risk factors identified were thoracolumbar kyphosis and a thoracoabdominal approach (for thoracolumbar pseudarthrosis), osteoarthritis of the hips and a positive sagittal balance ≥ 5 cm (for lumbosacral pseudarthrosis), and age > 55. As expected, the patients with pseudarthrosis had lower Scoliosis Research Society (SRS) scores than those with a solid fusion (71 vs. 90/120).
PRESENTATION
Pseudarthrosis can present in three different ways. The patient may be asymptomatic and have good function, they may be symptomatic, or they may have a pseudarthrosis associated with another pathological entity such as infection.
Functional Outcome Scores
It remains unclear why many patients with pseudarthrosis remain asymptomatic and have good functional outcomes. A small study from 1968 compared the outcomes of patients with solids fusion vs. pseudarthrosis and found little difference.21 The fusion description is given as either Hibbs or “H”-type, and it can be supposed therefore that the authors were performing uninstrumented fusions. A more modern study of uninstrumented fusions did not find the same results, with only 56% of patients with a pseudarthrosis achieving acceptable results compared to 86% of patients with a solid fusion.22
When looking at studies of instrumented fusions, there is mixed evidence of the correlation between solid union and good outcome. A review by Resnick et al. concluded that, “the majority of Class III medical evidence does suggest that successful radiographic fusion is associated with improved clinical outcomes.”23 Some of these studies were randomized but were still classified as Class III due to high crossover rates.
In an examination of consecutive deformity patients at one institution, all patients with a proven pseudarthrosis at one year or more all failed to improve their SRS or Oswestry Disability Index (ODI) scores.24 In fact, the lack of improvement in these scores was more accurate at detecting pseudarthrosis than plain X-rays. This was also noted in the scoliosis study discussed previously.20 This finding leads the authors to conclude that functional outcome scoring is essential to monitoring deformity patients postoperatively and should serve as a trigger for further investigation for pseudarthrosis.
Asymptomatic Pseudarthrosis
The detection of pseudarthrosis in the asymptomatic patient is usually as a result of surveillance by the surgeon and prompts an interesting consideration. For example, if a patient has a pseudarthrosis and yet is asymptomatic and functioning well, is anything to be gained by exposing them to radiation to find an anomaly that is most likely not going to require surgical intervention? Under what circumstances is the detection of a pseudarthrosis going to change the surgeon’s management of an asymptomatic patient? It would be reasonable that following any multilevel procedure or osteotomy, the early detection and treatment of an asymptomatic pseudarthrosis may prevent catastrophic complications in the future, and so therefore surveillance is reasonable. This can be done effectively and efficiently with standard scoring systems. Following a single level procedure, however, it is unlikely that there would be any major complication in the future even if it did not unite, so radiological screening is possibly less important.
Symptomatic Pseudarthrosis
In the case of symptomatic pseudarthrosis, the presentation is usually one of worsening axial back pain. The pain may be a worsening of the original pain of the operation (“never got better”) or may be new onset. Scoliosis patients may complain of worsening deformity although this is not common. In the case of Ankylosing Spondylitis, patients may be sensitive to their visual horizon. Neurological symptoms are unusual unless segmental deformity is considerable.
Concomitant Pseudarthrosis
The most likely concomitant diagnosis is infection. A history of fevers, unplanned return to the operating theatre, long term antibiotic therapy, and that of a discharging wound is strongly suggestive of infection. Weight loss and malaise may also accompany the presentation. Any other portals for infection should be examined.
INVESTIGATION
The investigation of a suspected pseudarthrosis should take into account likely differential or concomitant diagnoses. Although difficult to interpret initially, CRP and ESR should be examined, as should any other bloods suggestive of infection. The wound should be inspected and any soft tissue swelling or collection documented. Any fluid collection should be sampled and sent off for microscopy, culture and sensitivity testing. Even preoperative investigations can miss low grade infections, so the surgeon must be prepared in case purulent fluid is encountered upon revision.
Imaging Studies
Statistical Analysis
Any discussion of imaging studies, or any other diagnostic test for that matter, must include an appreciation of sensitivity and specificity, and 𝜅 (kappa) values. Any surgeon must be familiar with these terms, and how they can be used to guide our decision making. For the purposes of reading the text below, the tests are analyzed as trying to detect a fusion. Hence, sensitivity refers to the chance of correctly identifying a fusion while specificity refers to the chance of correctly identifying a pseudarthrosis.
A low sensitivity test may “miss” a solid fusion and may encourage the surgeon to perform unnecessary procedures in an attempt to fix an ostensible pseudarthrosis, which is actually solid. A low specificity test, on the other hand, may “miss” a pseudarthrosis and leave the surgeon and patient of the belief that the fusion is solid, when in fact it is not.
The kappa value, or Cohen’s kappa coefficient, is a measure of the agreement between observers and varies between 0 (no agreement, or agreement only by chance) and 1 (perfect agreement). A value of 0.41–0.60 is regarded as showing moderate agreement, and 0.61–0.80 substantial agreement. Values over 0.81 are regarded as “almost perfect” agreement in the biomedical fields.25 The practical significance of this is that even if a test has high sensitivity and specificity, a low kappa value should flag to the surgeon that the actual result can be heavily observer dependent. A way around this may be to obtain consensus by presentation of the results to multiple specialists.
X-rays
Plain X-rays
Two of the best studies looking at plain radiographs are those by Brodsky and Kant.26,27 Their results were fairly similar. Correlation between plain static X-rays and surgical exploration was 64–68%, with a sensitivity of 85–89% but a low specificity of 60–62%. If an X-ray demonstrates a solid fusion, in other words, then it is likely to be solid, but if it suggests pseudarthrosis, then it cannot be relied upon. Time from surgery to detection of a pseudarthrosis by X-ray is also quite long, with a mean of 3.5 years.20
Another issue is the large variability in interpreting X-rays, both inter- and intra-observer. In one study where X-rays were assessed by two surgeons and two radiologists, the 𝜅 = 0.4–0.7, indicating poor correlation. Therefore, despite the relative inexpensive nature of plain X-rays and their availability, the authors do not recommend them for the assessment of solid fusion.
Bending or Dynamic X-rays
Bending or dynamic films, also known as flexion-extension studies, perform similarly to plain X-rays when investigating pseudarthrosis. In the same study by Brodsky et al. referenced above, it was found that while an absence of motion on these studies correlated well with solid fusion, movement does not necessarily indicate pseudarthrosis.26
Computed Tomography (CT)
In the already discussed study by Brodsky et al., CT scanning was only found to have a sensitivity of 63%, specificity of 86%, positive predictive value of 72% and negative predictive value of 81%. These results were not dramatically different from plain X-ray, yet one must keep in mind that this study, and many like it, were performed in the late 1980s. It should come as no surprise, therefore, that more modern studies, with more modern helical multi-slice scanners, have shown much better results. Unfortunately, not many have compared the imaging to surgical exploration.
Posterolateral Fusions
Two more recent studies compared CT scan findings to surgical exploration. In their 2007 paper,28 Carreon et al. used 1 mm axial slice CT scans printed on film and had them assessed by three spine surgeons. Interestingly, they documented fusion across the facet joint as well as fusion in the posterolateral gutters. When fusion was seen in both facets and both posterolateral gutters, the chance of a solid fusion at exploration was 96%. If it was seen only in the posterolateral gutters then this dropped to 89%, and finally if there was only fusion seen across the facet joints, then the chance of seeing a solid fusion at exploration was 74%. However, the absence of fusion across both facet joints or one posterolateral gutter did not reliably predict pseudarthrosis on exploration.
Anterior Lumbar Interbody Fusions (ALIF)
In the second paper looking at anterior lumbar interbody fusions using metallic cages by Carreon et al.,29 a similar protocol was used. Although there was substantial variability amongst observers, when consensus was obtained, CT scan had a 93% sensitivity and a 46% specificity for fusion. The anterior sentinel sign30 only had a 20% sensitivity and 92% specificity for detecting a fusion, whereas the posterior sentinel sign proved to be more accurate, with 67% sensitivity and 79% specificity. The absence of an anterior sentinel sign is a good test for pseudarthrosis.
Posterior/Transforaminal Lumbar Interbody Fusions (PLIF/TLIF)
The assessment of interbody fusion is often problematic. Artefact can often interfere with CT imaging, particularly when performed on old machines, and tantalum markers within PEEK or carbon fiber cages can often leave a dramatic artefact (Fig. 4-1). Modern multi-slice helical machines with more sophisticated artefact removal algorithms have made the task much easier, and coronal plane reconstructions are excellent at visualizing the interbody fusion mass.
Shah et al.31 performed CT scans on patients 6 months postoperatively who had undergone a PLIF using titanium cages, where the only bone graft was packed within the cages. He described bridging bony trabeculation both within the cages, but also outside the cages where no bone graft had been packed. Similarities to the sentinel sign were noted. He also found that CT was far more sensitive at determining the presence or absence of a radiolucent endplate cage interface than X-ray, with very high agreement between observers. Fogel et al.,32 on the other hand, found that there was little difference between CT scans and X-rays when assessing fusion following PLIF. The difficulty with the paper though is that there were only four pseudarthrosis cases found at exploration out of 172 levels surgically explored. With such a low pseudarthrosis rate of 2.3%, sensitivity and specificity calculations can be strongly influenced with relatively small changes in detection.
A very useful paper by Kanemura et al.33 tracked radiographic changes over time. They examined 153 patients up to five years postoperatively following PLIF using local bone graft and iliac crest. They found that motion ≥ 5° on dynamic X-rays was maximal at one year, but then steadily decreased over time. Likewise, they found that, using X-rays and CT scanning, radiolucent zones around pedicle screws were also maximal at one year, but then resolved without surgical intervention by three to four years. Anterior bridging bone began to form at three months and then continued. Interbody bone graft volume tended to decrease by 6 months, but then increase again after two to three years.
With so many changes associated with pseudarthrosis present at the 6- to 12-month postoperative mark, this paper challenges the surgeon to delay surgical intervention for pseudarthrosis until at least two or three years have passed, as many changes will resolve without intervention. Are any of the changes associated with the eventual diagnosis of pseudarthrosis? The only predictor found was the presence of a radiolucent zone around the interbody cage of greater than 1 mm at 12 and 18 months. This was an independent predictor, and associated with subsidence, motion and decreasing interbody bone graft.
Magnetic Resonance Imaging
Although there have been some studies looking at the accuracy of MRI,34,35 it has not been compared favorably to CT or operative exploration. It may give the surgeon information about the Modic changes present across the fused disc space, but this hasn’t been shown to reliably correlate to fusion or pseudarthrosis.
Roentgen Stereophotogrammetric Analysis (RSA)
RSA is a technique whereby tantalum markers are embedded within the bony vertebrae at the time of surgery. Standardized imaging is then taken of the beads in the postoperative period, and movement can be measured accurately.36 This technique suffers a similar problem to that of dynamic X-rays, in that motion, or lack thereof, does not necessarily correlate to pseudarthrosis. For example, according to RSA there may be no motion across a segment immediately after the surgery, yet obviously no fusion has yet established.37 It is used for research purposes only, and clinical correlation to fusion should be made carefully.
Nuclear Medicine
Technetium-99m bone scanning is often used to assess the activity of bone around a fusion mass. It is thought to correlate to fusion as the scan is “cold”. Evidence of its usefulness is, however, lacking. When compared to surgical exploration, although it was specific (93%), it lacked sensitivity (50%) and only had a positive predictive value of 40% when looking for pseudarthrosis.38 Similar results were found when looking at scoliosis patients.39 It is thought that the chief problem is that the technique is unable to differentiate between established pseudarthrosis and immature fusion mass.
Ultrasound
The use of ultrasound has been evaluated in one small study, comparing the appearance of the posterior structures to surgical exploration.40 Although it appeared to be promising, it is limited in its ability to assess the anterior fusion mass. No further studies have been carried out.
CLASSIFICATION
Posterolateral Fusion
Heggeness and Esses were the first to classify morphologically different types of pseudarthrosis of posterolateral fusions (Table 4-1).41 They also described the “shingle sign” which is commonly seen in the shingle type of pseudarthrosis, in which a sliver of bone seen to be floating behind the posterior elements when looking at an axial CT slice. This classification is useful in that it is suggestive of the cause of the pseudarthrosis.
| Type | Description |
| Atrophic | atrophy and resorption of the fusion bone mass |
| Transverse | adequate bone mass but a horizontal discontinuity persists |
| Shingle | variation of the transverse where the discontinuity is oblique |
| Complex | the presence of multiple fusion defects |
Lenke et al.42 described a more qualitative classification of posterolateral fusion mass, ranging from A “definitely solid” to D “definitely not solid” (Table 4-2). While this may be useful to describe fusions, it does give the surgeon assistance in diagnosing or treating the complication.
| Type | Shorthand | Description |
| A | definitely solid | solid big trabeculated bilateral fusion masses |
| B | possibly solid | unilateral large fusion mass with contralateral small fusion mass |
| C | probably not solid | small, thin fusion masses bilaterally |
| D | definitely not solid | graft resorption bilaterally or fusion mass with obvious bilateral pseudarthrosis |
Interbody Fusion
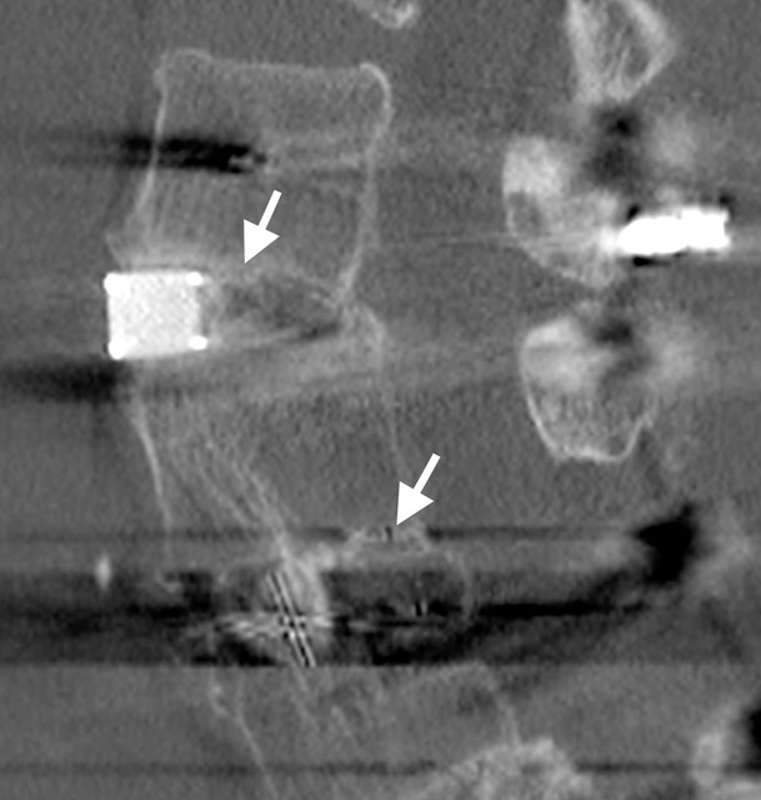
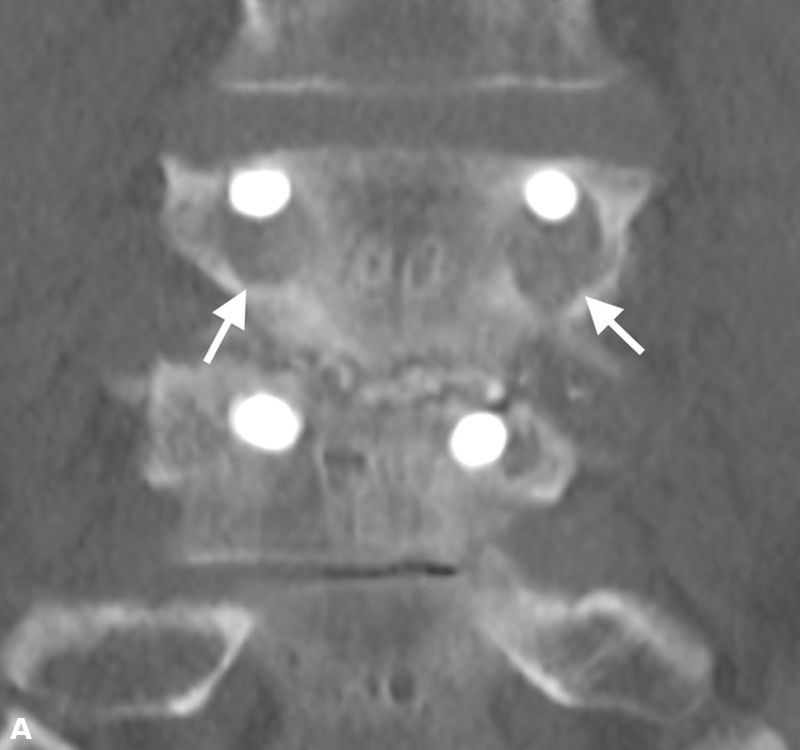
Brantigan and Steffee first described a classification of interbody fusion through their carbon fiber cage.43 Later modified by Fraser, it is usually known as the BSF (Brantigan, Steffee, Fraser) classification (Table 4-3).32,44 Pseudarthrosis is evaluated by CT scan, and classified as BSF-1 where there are gross signs of movement (Fig. 4-2), or BSF-2 where there is a horizontal lucency across the interbody space (Fig. 4-3). The latter is usually known as a “locked pseudarthrosis”. Regarding fusion, they regarded the fusion to be solid if bone was seen to grow through one of the PLIF cages, even if the other had lucency across it.
| Description | |
| BSF-1 | Radiographical pseudarthrosis is indicated by
|
| BSF-2 | Radiographical locked pseudarthrosis is indicated by lucency visible in the middle of the cages with solid bone growing into the cage from each vertebral endplate. |
| BSF-3 | Radiographical fusion: bone bridges at least half of the fusion area with at least the density originally achieved at surgery. |


SURGICAL STRATEGIES
The decision to offer surgical intervention always needs to be a balance of risks and benefits. An asymptomatic patient with a single level pseudarthrosis may not require intervention, but a patient with a long fusion, even if asymptomatic, may warrant consideration to avoid making future surgery much more difficult. It should be noted that, even after successful fusion, patients who had suffered from a pseudarthrosis do not do as well as those who had a successful fusion after their initial surgery.5
Approach
The variations in the surgical treatment of a pseudarthrosis are as many and varied as the methods of performing a fusion in the first place. The general principles to be followed are to improve stabilization, perform new grafting, and restore sagittal alignment.45 In order to improve stabilization, clearly loose and broken instrumentation should be replaced. Often pedicle screws can be “upsized” by a millimeter or two in diameter to achieve good grip in a previously loose screw trajectory. Lengthening screws is also sometimes possible but requires careful preoperative planning. Extending the fixation to an adjacent segment should be considered especially if it is associated with adjacent segment disease, but one needs to keep in mind that the newly incorporated levels also need to achieve fusion. In a practical sense, for a failed lumbosacral fusion, extending fixation to the ilium is often very effective at improving stabilization.46
The addition of interbody graft to a failed posterolateral fusion is a means of adding graft material under compression, as well as improving stabilization. By replacing a “soft” disc space with a relatively stiffer cage and graft combination, anterior column support is improved. Depending on the level, this may be performed either via an anterior or lateral approach. A TLIF or PLIF technique may also be used but these will most likely encounter scar tissue and increase the risk of nerve injury and dural tears.
Sagittal Balance
Sagittal balance always needs to be measured and accounted for. A patient with a pseudarthrosis in poor sagittal alignment will still have a poor outcome with a solid fusion if their alignment is not addressed. An osteotomy through a pseudarthrosis may be necessary to achieve correction, but once more, the surgeon must optimize the chance of fusion by achieving good bone apposition, stiff and strong constructs and by improving the patient’s own risk factors.
Stimulation
Some research exists to support the use of DC current stimulators,47,48 as well as pulsed electromagnetic field stimulation.49-51 Unfortunately, neither method has shown consistently good outcomes and has largely fallen out of widespread use.
Bone Graft
There is no synthetic substitute for iliac crest graft, and this should always be the source of graft material whenever it is available for the treatment of pseudarthrosis. While rhBMP-2 has been shown to be equivalent to autologous bone graft in two large systematic reviews,52,53 it is not without cost or complications. Allografts lack osteoinductive properties as do ceramics such as tricalcium phosphate, and when the surgeon is treating a pseudarthrosis, biologically inert “fillers” such as these should be avoided.
CONCLUSION
Pseudarthrosis is still one of the most challenging problems facing the spinal surgeon, and the risk of it should be discussed with all potential fusion patients. Minimization of the risks of pseudarthrosis begins well before scalpel touches skin, with preoperative investigations completed, planning performed, and all risk factors mitigated.
Any fusion patient that does not respond in the usual fashion should flag to the surgeon the possibility that pseudarthrosis is developing. The surgeon who “blames” the patient does not do their patient or themselves justice. Relevant investigations include X-rays and CT scans; subtle changes over time should be noted.
Once the diagnosis is established, careful and open discussion should occur regarding the benefits and risks of surgical intervention as this decision is not always clear. Once surgical intervention is decided upon, the surgeon must take into account the mode of failure as well as the necessary steps it will take to achieve fusion in an acceptable alignment. Unfortunately, the operative and postoperative course cannot be expected to be routine, and one must council the patient that they might never achieve the expected outcome from their index operation.
PEARLS AND PITFALLS
- In patients with a high risk of development of pseudarthrosis, plan and prepare to perform surgery that will mitigate those risks. Instrumentation improves fusion rate, as does performing 360° fusions either through two separate approaches, or with interbody as well as bilateral posterolateral grafts.
- Suspect a patient is developing a pseudarthrosis if their functional outcome scores do not improve as expected.
- Coronal plane CT scan reconstructions are the investigation of choice to find a pseudarthrosis, and, in particular, a “locked pseudarthrosis.”
- Loosening around screws should resolve with time and should be carefully followed, but lucency around an interbody cage is likely to be the precursor of an eventual pseudarthrosis.
- Autologous bone graft should be the grafting material of choice.
SUGGESTED READING
- Choudhri TF, Mummaneni PV, Dhall SS, et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 4: radiographic assessment of fusion status. J Neurosurg Spine. 2014;21(1):23-30.
- Lee C, Dorcil J, Radomisli TE. Nonunion of the spine: a review. Clin Orthop Relat Res. 2004;(419):71-75.
- Resnick DK, Choudhri TF, Dailey AT, et al. Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 4: radiographic assessment of fusion. J Neurosurg Spine. 2005;2(6):653-657.
REFERENCES
- Adogwa O, Parker SL, Shau D, et al. Cost per quality-adjusted life year gained of revision fusion for lumbar pseudoarthrosis: defining the value of surgery. J Spinal Disord Tech. 2015;28(3):101-105.
- Chun DS, Baker KC, Hsu WK. Lumbar pseudarthrosis: a review of current diagnosis and treatment. Neurosurg Focus. 2015;39(4):E10.
- Raizman NM, O’Brien JR, Poehling-Monaghan KL, Yu WD. Pseudarthrosis of the spine. J Am Acad Orthop Surg. 2009;17(8):494-503.
- Hadley MN, Reddy SV. Smoking and the human vertebral column: a review of the impact of cigarette use on vertebral bone metabolism and spinal fusion. Neurosurgery. 1997;41(1):116-124.
- Gertzbein SD, Hollopeter MR, Hall S. Pseudarthrosis of the lumbar spine. Outcome after circumferential fusion. Spine. 1998;23(21):2352-2356; discussion 2356-2357.
- Brown CW, Orme TJ, Richardson HD. The rate of pseudarthrosis (surgical nonunion) in patients who are smokers and patients who are nonsmokers: a comparison study. Spine. 1986;11(9):942-943.
- Bydon M, De la Garza-Ramos R, Abt NB, et al. Impact of smoking on complication and pseudarthrosis rates after single- and 2-level posterolateral fusion of the lumbar spine. Spine. 2014;39(21):1765-1770.
- Jenkins JD, Coric D, Branch CL Jr. A clinical comparison of one- and two-screw odontoid fixation. J Neurosurg. 1998;89(3):366-370.
- Deguchi M, Rapoff AJ, Zdeblick TA. Posterolateral fusion for isthmic spondylolisthesis in adults: analysis of fusion rate and clinical results. J Spinal Disord. 1998;11(6):459-464.
- Boden SD, Sumner DR. Biologic factors affecting spinal fusion and bone regeneration. Spine. 1995;20(24 Suppl):102S-112S.
- Bono CM, Lee CK. Critical analysis of trends in fusion for degenerative disc disease over the past 20 years: influence of technique on fusion rate and clinical outcome. Spine. 2004;29(4):455-463; discussion Z5.
- Zdeblick TA. A prospective, randomized study of lumbar fusion. Preliminary results. Spine. 1993;18(8):983-991.
- Nemoto O, Asazuma T, Yato Y, Imabayashi H, Yasuoka H, Fujikawa A. Comparison of fusion rates following transforaminal lumbar interbody fusion using polyetheretherketone cages or titanium cages with transpedicular instrumentation. Eur Spine J. 2014;23(10):2150-2155.
- Wu SH, Li Y, Zhang YQ, et al. Porous titanium-6 aluminum-4 vanadium cage has better osseointegration and less micromotion than a poly-ether-ether-ketone cage in sheep vertebral fusion. Artif Organs. 2013;37(12):E191-E201.
- Olivares-Navarrete R, Gittens RA, Schneider JM, et al. Osteoblasts exhibit a more differentiated phenotype and increased bone morphogenetic protein production on titanium alloy substrates than on poly-ether-ether-ketone. Spine J. 2012;12(3):265-272.
- Bridwell KH, Lewis SJ, Lenke LG, Baldus C, Blanke K. Pedicle subtraction osteotomy for the treatment of fixed sagittal imbalance. J Bone Joint Surg Am. 2003;85-A(3):454-463.
- Dickson DD, Lenke LG, Bridwell KH, Koester LA. Risk factors for and assessment of symptomatic pseudarthrosis after lumbar pedicle subtraction osteotomy in adult spinal deformity. Spine. 2014;39(15):1190-1195.
- Deviren V, Tang JA, Scheer JK, et al. Construct rigidity after fatigue loading in pedicle subtraction osteotomy with or without adjacent interbody structural cages. Global Spine J. 2012;2(4):213-220.
- Hyun SJ, Lenke LG, Kim YC, Koester LA, Blanke KM. Long-term radiographic outcomes of a central hook-rod construct for osteotomy closure: minimum 5-year follow-up. Spine. 2015;40(7):E428-E432.
- Kim YJ, Bridwell KH, Lenke LG, Rhim S, Cheh G. Pseudarthrosis in long adult spinal deformity instrumentation and fusion to the sacrum: prevalence and risk factor analysis of 144 cases. Spine. 2006;31(20):2329-2336.
- DePalma AF, Rothman RH. The nature of pseudarthrosis. Clin Orthop Relat Res. 1968;59:113-118.
- Kornblum MB, Fischgrund JS, Herkowitz HN, Abraham DA, Berkower DL, Ditkoff JS. Degenerative lumbar spondylolisthesis with spinal stenosis: a prospective long-term study comparing fusion and pseudarthrosis. Spine. 2004;29(7):726-733; discussion 733-734.
- Resnick DK, Choudhri TF, Dailey AT, et al. Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 5: correlation between radiographic and functional outcome. J Neurosurg Spine. 2005;2(6):658-661.
- Klineberg E, Gupta M, McCarthy I, Hostin R. Detection of pseudarthrosis in adult spinal deformity: the use of health-related quality-of-life outcomes to predict pseudarthrosis. Clin Spine Surg. 2016;29(8):318-322.
- Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174.
- Brodsky AE, Kovalsky ES, Khalil MA. Correlation of radiologic assessment of lumbar spine fusions with surgical exploration. Spine. 1991;16(6 Suppl):S261-S265.
- Kant AP, Daum WJ, Dean SM, Uchida T. Evaluation of lumbar spine fusion. Plain radiographs versus direct surgical exploration and observation. Spine. 1995;20(21):2313-2317.
- Carreon LY, Djurasovic M, Glassman SD, Sailer P. Diagnostic accuracy and reliability of fine-cut CT scans with reconstructions to determine the status of an instrumented posterolateral fusion with surgical exploration as reference standard. Spine. 2007;32(8):892-895.
- Carreon LY, Glassman SD, Schwender JD, Subach BR, Gornet MF, Ohno S. Reliability and accuracy of fine-cut computed tomography scans to determine the status of anterior interbody fusions with metallic cages. Spine J. 2008;8(6):998-1002.
- McAfee PC. Interbody fusion cages in reconstructive operations on the spine. J Bone Joint Surg Am. 1999;81(6):859-880.
- Shah RR, Mohammed S, Saifuddin A, Taylor BA. Comparison of plain radiographs with CT scan to evaluate interbody fusion following the use of titanium interbody cages and transpedicular instrumentation. Eur Spine J. 2003;12(4):378-385.
- Fogel GR, Toohey JS, Neidre A, Brantigan JW. Fusion assessment of posterior lumbar interbody fusion using radiolucent cages: X-ray films and helical computed tomography scans compared with surgical exploration of fusion. Spine J. 2008;8(4):570-577.
- Kanemura T, Matsumoto A, Ishikawa Y, et al. Radiographic changes in patients with pseudarthrosis after posterior lumbar interbody arthrodesis using carbon interbody cages: a prospective five-year study. J Bone Joint Surg Am. 2014;96(10):e82.
- Kröner AH, Eyb R, Lange A, Lomoschitz K, Mahdi T, Engel A. Magnetic resonance imaging evaluation of posterior lumbar interbody fusion. Spine. 2006;31(12):1365-1371.
- Lang P, Chafetz N, Genant HK, Morris JM. Lumbar spinal fusion. Assessment of functional stability with magnetic resonance imaging. Spine. 1990;15(6):581-588.
- Johnsson R, Selvik G, Strömqvist B, Sundén G. Mobility of the lower lumbar spine after posterolateral fusion determined by roentgen stereophotogrammetric analysis. Spine. 1990;15(5):347-350.
- Johnsson R, Axelsson P, Gunnarsson G, Strömqvist B. Stability of lumbar fusion with transpedicular fixation determined by roentgen stereophotogrammetric analysis. Spine. 1999;24(7):687-690.
- Bohnsack M, Gossé F, Rühmann O, Wenger K. The value of scintigraphy in the diagnosis of pseudarthrosis after spinal fusion surgery. J Spinal Disord. 1999;12(6):482-484.
- McMaster MJ, Merrick MV. The scintigraphic assessment of the scoliotic spine after fusion. J Bone Joint Surg Br. 1980;62-B(1):65-72.
- Jacobson JA, Starok M, Pathria MN, Garfin SR. Pseudarthrosis: US evaluation after posterolateral spinal fusion: work in progress. Radiology. 1997;204(3):853-858.
- Heggeness MH, Esses SI. Classification of pseudarthroses of the lumbar spine. Spine. 1991;16(8 Suppl):S449-S454.
- Lenke LG, Bridwell KH, Bullis D, Betz RR, Baldus C, Schoenecker PL. Results of in situ fusion for isthmic spondylolisthesis. J Spinal Disord. 1992;5(4):433-442.
- Brantigan JW, Steffee AD. A carbon fiber implant to aid interbody lumbar fusion. Two-year clinical results in the first 26 patients. Spine. 1993;18(14):2106-2107.
- Santos ER, Goss DG, Morcom RK, Fraser RD. Radiologic assessment of interbody fusion using carbon fiber cages. Spine. 2003;28(10):997-1001.
- Larsen J, Capen DA. Pseudarthrosis of the lumbar spine. J Am Acad Orthop Surg. 1997;5(3):153-162.
- Kuklo TR, Bridwell KH, Lewis SJ, et al. Minimum 2-year analysis of sacropelvic fixation and L5-S1 fusion using S1 and iliac screws. Spine. 2001;26(18):1976-1983.
- Tejano NA, Puno R, Ignacio JM. The use of implantable direct current stimulation in multilevel spinal fusion without instrumentation. A prospective clinical and radiographic evaluation with long-term follow-up. Spine. 1996;21(16):1904-1908.
- Goodwin CB, Brighton CT, Guyer RD, Johnson JR, Light KI, Yuan HA. A double-blind study of capacitively coupled electrical stimulation as an adjunct to lumbar spinal fusions. Spine. 1999;24(13):1349-1356; discussion 1357.
- Hodges SD, Eck JC, Humphreys SC. Use of electrical bone stimulation in spinal fusion. J Am Acad Orthop Surg. 2003;11(2):81-88.
- Simmons JW. Treatment of failed posterior lumbar interbody fusion (PLIF) of the spine with pulsing electromagnetic fields. Clin Orthop Relat Res. 1985;(193):127-132.
- Simmons JW Jr, Mooney V, Thacker I. Pseudarthrosis after lumbar spine fusion: nonoperative salvage with pulsed electromagnetic fields. Am J Orthop. 2004;33(1):27-30.
- Simmonds MC, Brown JV, Heirs MK, et al. Safety and effectiveness of recombinant human bone morphogenetic protein-2 for spinal fusion: a meta-analysis of individual-participant data. Ann Intern Med. 2013;158(12):877-889.
- Fu R, Selph S, McDonagh M, et al. Effectiveness and harms of recombinant human bone morphogenetic protein-2 in spine fusion: a systematic review and meta-analysis. Ann Intern Med. 2013;158(12):890-902.