
Adriaan Hendrik Botha and Robert N. Dunn
CORE CURRICULUM
Introduction
- What is the incidence of gunshot injuries to the spine?
- What is the epidemiology of gunshot injuries to the lumbar spine?
- What are the cost implications of these injuries?
How were these injuries managed previously?
Describe the ballistics of gunshot injuries
- How do we define high- versus low-energy injuries?
- Determining the kinetic energy of a bullet
- Does bullet design play a role in the injury?
- What is the temporary and the permanent cavity?
How do we clinically evaluate a patient with a gunshot injury?
- The importance of ATLS principles.
- What other associated injuries can there be?
What imaging should be requested?
- Which xrays must be performed?
- What is the role of CT scans?
- MRI dangerous with the bullet in the canal?
Does there need to be concern regarding lead toxicity?
- What is the incidence of lead toxicity?
- What are the symptoms of plumbism?
- How do you treat lead toxicity?
Fracture stability
- How do we assess stability?
Neurological Injury
- How common is neurological injury?
- Do steroids provide any benefit?
- What is the prognosis of recovery?
Removal of bullets and retained fragments
- When must bullets be removed?
- What are the complications of bullet removal?
Gunshot injuries to the Cauda Equina
- What is the challenge with gunshot injuries to the cauda equine?
- Do we need to remove bullet fragments from the cauda equine?
Antibiotics and wound management
- What antibiotics should be administered?
- How long should it be administered?
- Do we need to remove transabdominal bullet fragments lodged in the spine?
Introduction
What is the incidence of gunshot injuries to the spine?
- 17% of all spinal cord injuries in the USA are due to gunshot wounds.
- Statistics relating to lumbar spine gunshot injuries specifically are difficult to get.
- Groote Schuur Hospital in Cape Town reported 120 gunshot injuries per month.
- Chris Hani Baragwanath Hospital’s incidence increased from 988 cases in 1988 to 3152 cases in 1998.
What is the epidemiology of gunshot injuries to the spine?
- Most common are males aged 15–34 years.
- High incidence of complete neurological injuries.
What are the cost implications of these injuries?
- Average hospital stay ranges from 58–85 days.
- Cost associated per case including in-patient rehabilitation, $87,750-$142,710.
- High incidence of associated injuries driving further cost (Fig. 9-1).

How were These Injuries Managed Previously?
- When Lord Nelson sustained a spinal cord injury from a gunshot at the Battle of Trafalgar his personal surgeon told him, “My Lord, unhappily for our country, nothing can be done for you.” Nelson died a few hours later.
- Majority of literature pertains to military gunshot and shrapnel injuries, not to civilian gunshot injuries, due to the high energy nature of it. Military protocols are both expensive and resource intensive.
- Treatment of military spinal gunshot wounds entails debridement of all contaminated tissue along the tract and removal of bony and bullet fragments from the spinal canal, closure of dural defects to prevent fistulas and surgical decompression of the spinal cord.
- Same treatment protocol does not apply to civilian gunshot wounds due to the lower energy of the projectiles.
- Incidence of civilian gunshot wounds due to military type rifles are on the increase, often needing treatment protocols as dictated for high-energy wounds.
- Literature regarding civilian gunshot injuries is dated.
Describe the Ballistics of Gunshot Injuries
How do we define high- versus low-energy injuries?
- Traditionally described as high (>2000 ft/sec) or low velocity (<2000 ft/sec). Recent trend towards terms high- versus low-energy. This does not describe injury patterns adequately.
- Shotgun is a low velocity weapon, although extreme energy amounts are transferred to soft tissue.
Determining the kinetic energy of a bullet
- Amount of energy transferred is calculated by formula KE = 0.5 x m x v2.
KE = Kinetic energy
M = mass of projectile
V = velocity
- Difference between entry and exit kinetic energy is the amount of energy transferred to soft tissue. If the exit velocity is 0, then all the energy was transferred to the soft tissue.
- A 9mm bullet of 115 grain weight has 401 ft/pound muzzle energy when it leaves the barrel.
- A M16 5.56mm round has 1297 ft/pound muzzle energy (Fig. 9-2).
- A 12-gauge shotgun slug has 2604 ft/pound muzzle energy, although the velocity is only 1180 feet/second, which classifies it as a low velocity weapon (Fig. 9- 3).
- Energy transfer also depends on bullet design, entry profile, projectile stability and the density of tissue it transverses (Fig. 9-4).


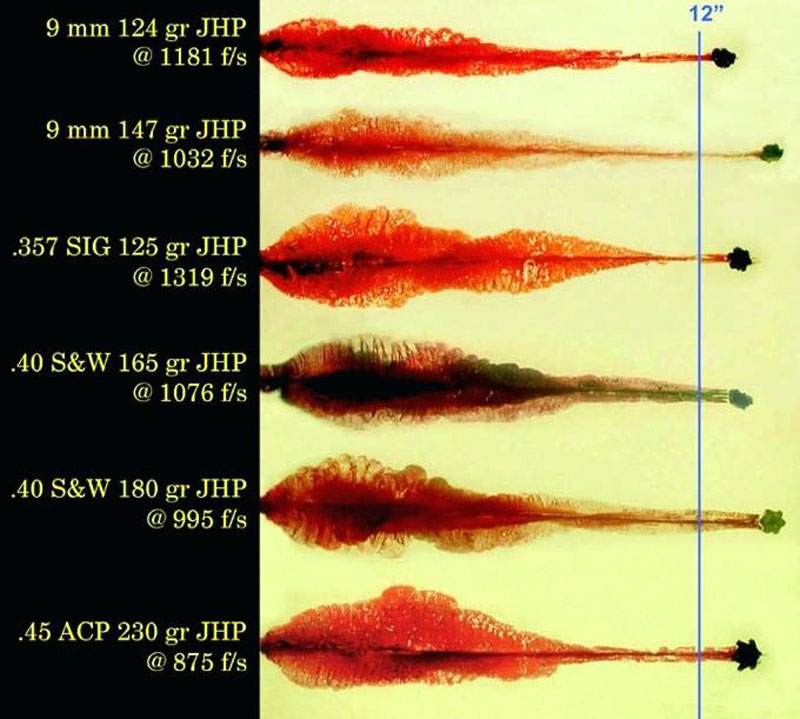
Does bullet design play a role in the injury?
- Design of bullets dictates amount of energy transferred.
- Full metal jacket bullets are designed to maintain maximum amount of energy by resisting deformation.
- Hollow-point ammunition deforms and fragments very easily, transfering greater amounts of energy to soft tissue causing more damage.
- The majority of bullets contain a lead core with a copper or nickel jacket.
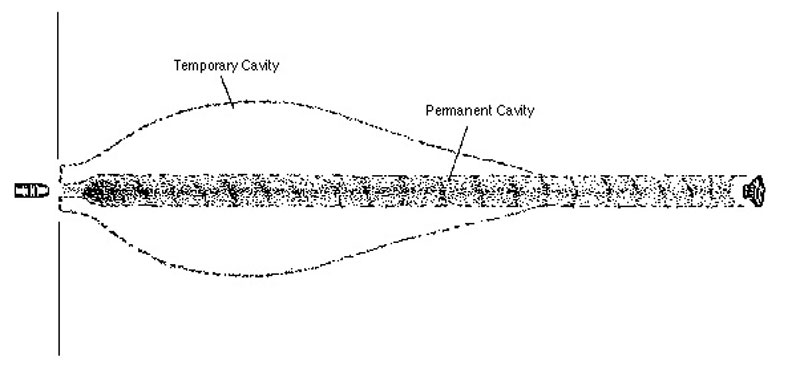
What is the temporary and the permanent cavity?
A bullet traversing soft tissue causes injury by one of two mechanisms.
- First, the permanent cavity is created by the bullet itself. The extent of the permanent cavity depends on the size of the bullet and the position of the bullet when it strikes soft tissue i.e. yaw.
- Second, the temporary cavity causes tissue damage via the shockwave created by the traversing bullet. It can be up to three times the size of the permanent cavity (Fig. 9-5). Factors that influence the size of the temporary cavity is the shape of the bullet and the speed at which it travels.
How Do We Clinically Evaluate a Patient with a Gunshot Injury?
- Assessment should always be according to Advanced Trauma Life Support (ATLS) principles.
- Incidence of associated injuries varies between 79–280%, with the vast majority abdominal injuries.
- It is of utmost importance to evaluate these patients along with other specialities according to ATLS principles and not to see the spinal gunshot injury as an isolated entity.
- 65% of these associated injuries will need surgical intervention.
What Imaging Should Be Requested?
Cover entry and exit wounds with radiopaque marker, i.e. electrocardiogram (ECG) sticker. This identifies the tract of the bullet and what organs are affected. This will dictate the imaging required. Bullets do not always travel in a straight line and can ricochet if they hit bone.
What xrays should be requested?
- Orthogonal views should be requested of affected structures (Fig. 9-6).
- Supplement with CT if xray does not yield sufficient visualization.
What is the role of CT scans?
CT will define bony detail of the injury and can aid in defining stability of fractures (Fig. 9-7).

Is an MRI dangerous with a bullet in the spinal canal?
- Magnetic resonance imaging of the spinal column with retained bullet fragments remains controversial.
- Shrapnel migration and the heating of residual fragments are the main concern.
- Dedini et al. showed that MRI Imaging of the spine with retained bullet fragments is safe, even up to 7 Tesla.1
- Fragment migration and bullet heating was not a concern.
- Stainless steel is only found in pellets and certain military ammunition and should not be of concern in civilian gunshot injuries, unless the projectile originates from a pellet gun or shotgun.
Do We Need To Be Concerned about Lead Toxicity?
What is the incidence of lead toxicity?
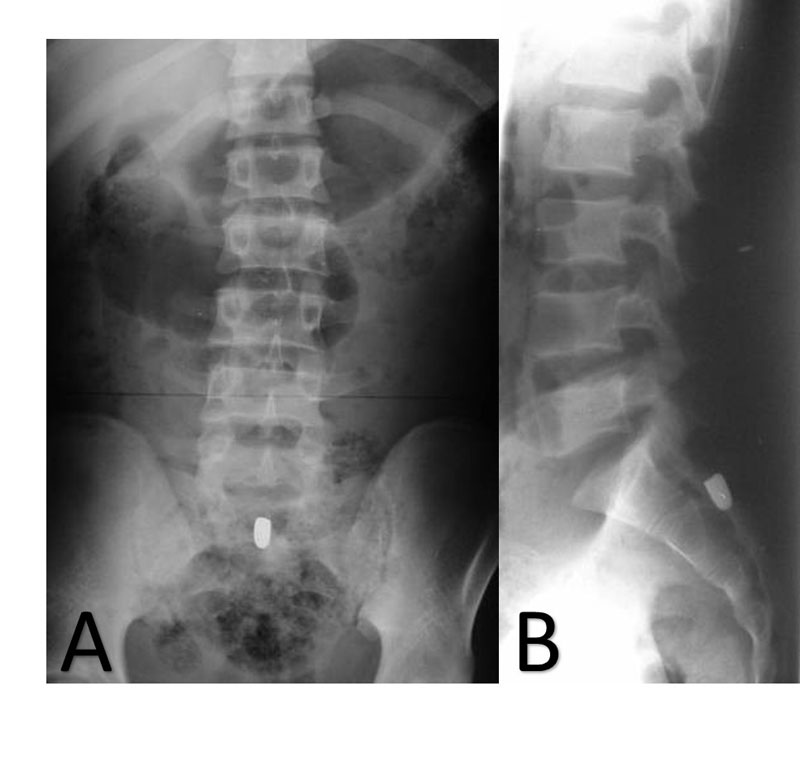
- Lead toxicity is more common when bullets are bathed in synovial fluid such as in the knee or hip.
- Very few cases report plumbism from bullets retained in spinal canal or disc space (Fig. 9-8).
- Lead toxicity should not be a concern or a reason for removal of the bullet.

What are the symptoms of plumbism?
Clinical picture of lead poisoning includes hypertension, abdominal cramping, constipation, joint and muscle pain, headache and mood disorders.
How do you treat lead toxicity?
- The treatment of lead poisoning is to, firstly, remove the source and to treat the patient with chelation therapy that binds and excretes the lead.
- Intra-dural copper fragments exhibit neural toxicity but not when extradural.
Fracture Stability
How do we assess fracture stability?
- Majority of the fracture classification system describes indirectly applied forces to the spinal column.
- Gun shot wounds (GSWs) are direct and directional forces and do not fit into classification systems.
- Even three column injuries can be stable in low energy gunshot injuries.
- Majority of civilian gunshot injuries are stable injuries.
- Any angulation or listhesis should further be evaluated for instability with flexion and extension radiographs (Fig. 9-9).
- If the bullet traversed both pedicles in the coronal plane, there is a risk of instability, and dynamic investigations should be performed.
- The majority of reported instability is secondary to surgical decompression.

Neurological Injury
How common is neurological injury?
- Neurological injury is common; the majority of injuries occur at the thoracic level.
- 25-59% result in complete spinal cord injuries, most common in the thoracic area.
Do steroids provide any benefit?
- No benefit identified by the administration of steroids for patients with neurological deficit, as also reported in the National Acute Spinal Cord Injury Study (NASCIS) trials.
- Administration of methylprednisolone had a high incidence of pancreatitis, while dexamethasone had the highest gastrointestinal (GIT) complication rate.
What is the prognosis for recovery?
Outcome and potential for recovery depends on the initial injury, and surgical intervention did not alter neurological outcome, in either complete or incomplete patients. Patients with incomplete neurology with preservation of neurological function distal to the level of injury did not improve.
- This still holds true today, except for patients with incomplete neurology with retained bullet fragments between T12 – L4 in the region.
- Patients that received decompressive surgery for bullet removal with incomplete injuries have a very high rate of complications and post-operative instability.
Removal of Bullets and Retained Fragments
When must bullets be removed?
- Current evidence shows that improvement in neurological status occurs only after removal of retained bullet fragments between the levels of T12 and L4 in patients with incomplete neurological deficit.
- Waters et al. showed no improvement in neurological status at any other level, regardless of being a complete or an incomplete injury.2
- The only indications for removal of retained bullet fragments would be progressive neurological deterioration, sepsis, lead poisoning and retained fragments between T12–L4 with incomplete neurological injury.
What are the complications of bullet removal?
- High complication rate associated with surgical removal of the retained fragments.
- Complications ranges from sepsis and cerebrospinal fluid (CSF) leaks post-operatively, to late instability.
- Robertson and Simpson found no benefit from removing bullet fragments.3
Gunshot Injuries to the Cauda Equina
What is the challenge with gunshot injuries to the cauda equine?
- Gunshot injuries to the cauda equina area present their own challenges. Due to the capacious canal, there is a tendency for bullets or fragments to migrate.
- Pre- and intra-operative fluoroscopic screening essential in cases where the bullet fragment will be removed.
- Bullet migration can happen independent from the location of the bullet, be it extra or sub-dural. It can also migrate in any direction.
Do we need to remove bullet fragments from the cauda equina?
- Stauffer reported a 94% improvement in patients that were treated non-operatively for gunshot wounds to the cauda equina.4
- Benzel et al. study showed similar rate of improvement in neurology, regardless of whether or not surgery was performed.5
Antibiotics and Wound Management
What antibiotics should be administered?
- Tetanus prophylaxis should be administered in all spinal gunshot injuries if there is doubt about immunization status.
- Broad spectrum antibiotics such as cephalosporin should be administered, but the duration of administration should be guided by the amount of soft tissue damage.
- Low rate of spinal and paraspinal sepsis in patients treated for 48hrs with a second generation cephalosporin.
For how long should broad spectrum antibiotics be administered?
- If there is no evidence of viscus perforation, 48–72hours should be sufficient.
- Antibiotic treatment of transabdominal gunshot injuries to the spine is a topic of debate.
- Spinal and paraspinal infections have been reported in patients treated with both extended or short course prophylaxis.
- Kumar et al. reported no spinal infection in their series of 13 patients with trans-colonic injuries who were treated with 7 days of prophylactic antibiotics.6
- High percentage of patients will develop infections in the gastro-intestinal tract due to the gunshot injury. These infections must be treated on their merit.
Do we need to remove transabdominal bullet fragments lodged in the spine?
- It is not deemed necessary to remove retained fragments.
- Missile tracts were not routinely irrigated in any of the studies, with no associated risk of developing spinal sepsis.
- Should laparotomy be indicated for intra-abdominal injury, it is advisable to irrigate the missile tract.
CONCLUSION
- Civilian gunshot injuries to the spinal column are increasing.
- Patients with associated spinal cord injury have a high morbidity due to associated injuries and require prolonged in-hospital treatment and rehabilitation.
- Current literature is aimed at the treatment of high energy gunshot injuries such as in war scenarios.
- Few current studies pertain to civilian gunshot injuries of the spinal column and their treatment.
- The only indications for removal of retained bullet fragments would be progressive neurological deterioration, sepsis, lead poisoning and retained fragments between T12–L4 with incomplete neurological injury.
- Routine irrigation and removal of the bullet fragments that traverse the abdomen is not necessary, unless the intra-abdominal injury warrants exploration.
- Duration of prophylactic antibiotic treatment has also been reduced, and spinal sepsis is an uncommon occurrence.
SUGGESTED READING
- Bartlett CS, Helfet DL,Hausman MR, Strauss E. Ballistics and gunshot wounds: effects on musculoskeletal tissues. J Am Acad Orthop Surg. 2000;8(1):21-36.
- Bumpass DB, Buchowski JM, Park A, et al. An update on civilian spinal gunshot wounds: treatment, neurological recovery, and complications. Spine (Phila Pa 1976) 2015;40(1):450-461.
- Farmer JC, Vaccaro AR, Balderston RA, Albert TJ, Cotler J. The changing nature of admissions to a spinal cord injury center: violence on the rise. J Spinal Disord. 1998;11(5):400-403.
- Stefanopoulos P, Pinialidis D,Hadjigeorgiou, Filippakis KN. Wound ballistics 101: the mechanisms of soft tissue wounding by bullets. Eur J Trauma Emerg Surg. 2017:43(5):579-586.
REFERENCES
- Dedini RD, Karacozoff AM, Shellock FG, Xu D, McClellan RT, Pekmezci M. MRI issues for ballistic objects: information obtained at 1.5-, 3- and 7-Tesla. Spine J. 2013;13(7):815-822.
- Waters RL. Gunshot wounds to the spine: the effects of bullet fragments in the spinal canal. J Am Paraplegia Soc. 1984;7(2):30-33.
- Robertson DP, Simpson RK. Penetrating injuries restricted to the cauda equina: a retrospective review. Neurosurgery. 1992;31(2):265-269.
- Stauffer ES, Wood RW, Kelly EG. Gunshot wounds of the spine: the effects of laminectomy. J Bone Joint Surg Am. 1979;61(3):389-392.
- Benzel EC, Hadden TA, Coleman JE. Civilian gunshot wounds to the spinal cord and cauda equina. Neurosurgery. 1987;20(2):281-285.
- Kumar A, Wood GW 2nd, Whittle AP. Low-velocity gunshot injuries of the spine with abdominal viscus trauma. J Orthop Trauma. 1998;12(7):514-517.