
Thomas Zweig and Ulrich Berlemann
INTRODUCTION
According to the United Nation’s World Health Organization (WHO), osteoporosis is among the ten most important “world diseases.” The extent of this problem is not only due to fractures of the peripheral skeletal system (neck of femur and the wrist), but even more due to fractures of the spine.
These fractures increase morbidity and mortality as they cause severe debilitating back pain and adversely affect quality of life, physical function and psychosocial performance. The treatment of vertebral compression fractures (VCF) of the thoracolumbar spine is challenging due to the broad variety of treatment options. Furthermore, treatment of osteoporosis, the cause itself, is more stratified, and, therefore, it is often a neglected part of the integral treatment.
Due to an aging population, osteoporotic vertebral fractures are becoming more frequent. Hence, a differentiated approach in treating the fractures is required. Choosing the most suitable method, from conservative to surgical, from minimally invasive (percutaneous vertebral augmentation procedures) to more invasive methods, is still not defined with common guidelines. In the following chapter, you will find an update on vertebral augmentation techniques.
EPIDEMIOLOGY
Due to various methodological approaches from different countries to collecting medical data on a larger scale, it remains difficult to acquire exact data on osteoporotic fractures of the spine. On the other hand, it is evident that the VCFs are a rising problem in industrialized and newly industrialized countries, which is mainly due to the shift in the demographic distribution towards the aged population. Accurate population data are easier to acquire as opposed to detailed data on VCF: worldwide birth rates have declined from 5 births per woman in the 1950s to 2.5 in the 2000s, and a further decrease is expected over time. On the other hand, life expectancy at birth has increased from 46.5 years in 1950 to 66 years in 2000.1 In 2010 in 12 countries, 5.2 million non-traumatic fractures were estimated to have been studied, of which 2.8 million were at the hip or spine. Other analyses showed that VCF accounted for almost as many fractures as the hip (NOF, neck of femur) and wrist (distal radius fractures) together.
Women accounted for most of the total non-traumatic fracture burden (77%).2 Osteoporotic vertebral fractures have a 39% prevalence in patients over the age of 65 years.3 They typically result in a wedge shape vertebra, causing local kyphosis, which may progress to a more severe kyphotic deformity following fracture of adjacent vertebrae.
Current Trends and Contradictory Study Results of the Past
Although numbers are currently rising, osteoporotic fracture of the thoracolumbar spine is not a new entity. It has been well diagnosed through x-ray diagnostics, but treatment options remain sparse. Previously bed rest or even plaster bed, tugging, physical therapy and analgesics were the only treatment options.
In 1987, Galibert et al. describe the percutaneous injection of bone cement (polymethyl methacrylate (PMMA)) to a vertebral angioma.4 Since that time, the method has developed and gained widespread acceptance and application. However, with the advancement from “simple” vertebroplasty (VP) to kyphoplasty, the costs rose exponentially, and criticism for the technique increased. Hence, in 2009, a climax was reached when two RCTs claimed to prove that there was no superiority of vertebroplasty over a sham procedure.5,6 However, the main weaknesses of these studies were the low cement volume and the inclusion of subacute fractures with pain for 3-12 months, among others. Despite the precise methodology of the studies and the unfavorable results, little has changed in the day-to-day practice of treating patients. Time has passed by, and the turmoil caused by these two studies that reported no benefit of VP versus sham has settled down. Meanwhile, the literature has shown superior results for minimally invasive transpedicular methods over nonsurgical treatment (FREE, VERTOS II, VAPOUR).7-9
Diagnostic Work Up
Radiography, standing x-ray a.p. and lateral
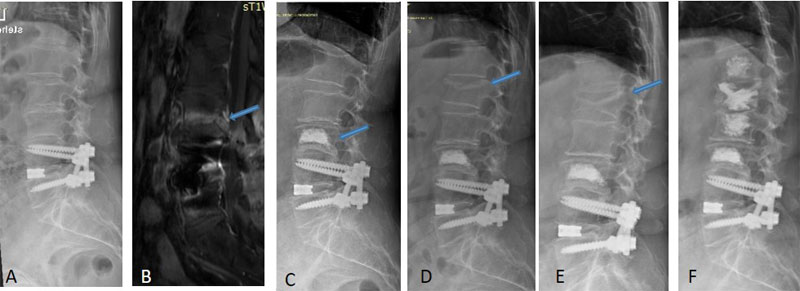
Standard standing x-ray imaging (Fig. 6-1A, B), initially, gives vital information about bony anatomy, identifying fractures and defining the fracture type, and, furthermore, the extent of lesions can be estimated. The initial planning of percutaneous transpedicular vertebral augmentation (pedicles) could be performed.

Magnetic resonance imaging (MRI)
Additional MRI imaging should be regarded as a gold standard diagnostic measure as it gives information about the bone biology. Only in rare cases can ambiguous signalling be found in the standard sequences t2, t1, STIR or TIRM (Fig. 6-2B) but in general acute, subacute, non-healed and old/healed fractures can be diagnosed well. Malignant infiltration is detected and infectious situations can be ruled out with high reliability.
Tc99m-bone-scan
In situations where MRI imaging is not possible (for example, due to a pacemaker, metallic fragments in the eye, pumps, claustrophobia), a bone scan answers questions about the age of the fracture and the levels that require treatment, as well as providing “biological” information.
Bolster x-ray lateral
Lordotic stress imaging with a bolster in the region of the fracture gives additional information regarding the mobility of the fracture. Especially in cases of a vertebra plana or Kümmel’s disease, persistent "mobility" of the fracture can be identified. Furthermore this valuable study simulates the lordotic positioning in the OR and shows the potential of vertebral height restoration preoperatively, in case of an existing mobility.
Computed tomography (CT)
In cases where fracture morphology remains unclear, and where there are doubts about clefts, and the patient would be put under risk of cement leakage to the spinal canal, the authors suggest additional CT-scans of the fracture region (limited CT).
Nonsurgical Therapy
As briefly outlined above, conservative therapy has been the only option for decades. It was comprised of bed rest and the plaster bed, and then, with the evolution of safe narcotic analgesics, early mobilization and bracing became increasingly popular. Early physiotherapy should be applied. This treatment regime is administered for several weeks. Although 50% of patients have shown good pain relief, this natural course can also conclude in insufficient pain relief at the 1-year follow up. Analgesic medication is very common, and physiotherapy has shown superior results over other conservative options.10
Minimally Invasive Percutaneous Therapy
In well-selected cases, there is no doubt that minimally invasive transpedicular options are bringing relief to patients with symptomatic osteoporotic fractures. A structured decision-making process, which still remains a challenge, is necessary in order to select the most suitable patients.
Over the years a clinical pathway has been developed, similar to that shown in Figure 6-3. This scheme incorporates both mechanical pain and deformity. First, a conservative therapy attempt should be undertaken, depending on the level of pain and the disability, in an out- or inpatient setting. In some countries, a specific period of conservative treatment is mandatory. Otherwise, an intervention is not reimbursed. A strict period of a mandatory conservative treatment interval can be regarded as disputable.

Regardless of the length of conservative treatment, it has been shown that patients with higher baseline pain (pain before surgery) have a greater benefit after surgery,11 and patients with painful vertebral compression fractures refractory to medical treatment are candidates for a cement augmentation. Further indications are symptomatic vertebra plana or instable osteonecrosis (Kümmel’s disease), stable A1 and A3 traumatic fractures,12 and malignancy (metastasis, lymphoma, multiple myeloma).
When looking at different spinal regions, procedures performed on the thoracolumbar junction (T11-L2) have more favorable outcomes than surgeries to the other segments (T5-T10 and L3-L5).8 There are relative and absolute contraindications, such as stable wedge of the vertebra/absence of further subsidence, tolerable kyphotic angle, asymptomatic patient, infectious conditions, blood-thinning agents, diffuse idiopathic skeletal hyperostosis (DISH) or ankylosing spondylitis (AS) with a suspected 3-column injury.
Figure 6-1A, B preoperative and Figure 6-1E, F postoperative are documenting a standard case.
Complications
When referring to commercial standardized informed consent forms, vital complications have to be specifically mentioned, because, even in the hands of experienced surgeons, severe events are encountered although they are rare. In general, there are two main reasons for adverse events:
(1) Instruments (K-wire, Jamshidi Needle, cannula) leaving the vertebral body anteriorly/posteriorly or medially/laterally can cause mechanical injury to or organs and/or neurostructures (such as the vena cava, aorta, pericardium/heart, lungs and the myelon/thecal sac) followed by organ specific complications.
(2) PMMA accessing the venous and the arterial system or leaving the anatomical borders of the vertebral body. Cement emboli are frequent, and, at the moment of cement application, hypotension has been observed. Fortunately, these observations are of clinical relevance rarely but the prevalence of these findings is up by 25%.7As in all operations, post interventional infection (0.5%) is a threat and could lead in the worst case to a major revision with corporectomy.13
Adjacent Segment Fractures
After the intensive application of both standard methods (Balloon Kyphoplasty (BKP) and VP) of cement augmentation of osteoporotic vertebral body fractures, many new fractures have been observed (Fig. 6-2C-E). There are many possibilities for the cause of this situation. Is this due to the stiffness of the cement-augmented vertebra? Is there a difference between BKP and VP? Or, is there no true difference at all in comparison to the natural course of the progressive fracturing spine? Are more fractures detected because surgical patients are more closely followed post-treatment than the conservatively treated cohort?
At the moment, conflicting results are reported in the literature:
(1) The risk for fractures is increased.14
(2) There is no increased risk for adjacent fractures.15 and
(3) With the weakest level of evidence, the risk of adjacent fractures is decreased.16
With a high level of evidence, a recent systematic review found that there was no increased risk for adjacent level fractures compared to conservative therapy of osteoporotic vertebral compression fracture (OVCF).17 The procedure (BKP/VP) itself does not seem to be the only determinant for an adjacent level fracture. The following variates have to be considered for the estimation of the risk of developing an adjacent segment fracture: including age, gender, bone mineral density (BMD), local kyphotic angle and number of pre-existing fractures before specific therapy.
Two risk factors, biology and biomechanics, should be considered carefully. There is a consensus that highly decreased BMD (biology) is a key factor for further fractures, whether treated with cement augmentation or conservatively. A measurement of BMD should always be initiated after a first OVCF. If there was none before, start with the treatment of the systemic reason for the fracture. Sufficient treatment of osteoporosis (OP) reduces the risk of adjacent fractures.
Considerations of stiffness, change of elasticity module, stress loading/distribution and sagittal profile/sagittal alignment (biomechanics) are important. There seems to be reduced stress on endplates of a neighboring vertebra in BKP as the cavity leaves more remaining trabecular bone under the endplate of the cement filled VP. Following this concept, more stress can be observed on the adjacent endplate if the cement is positioned in proximity to the endplate of the treated VP (cement positioning). The cement volume injected is related to this; a 30% filling restores the previous stiffness. Overfilling might increase the rate of adjacent fractures.
The current global view on the whole spine with the concept of sagittal balance opens a broader view on the biomechanics of OVCF. Hence, it is of importance to reduce the fracture to diminish the effect of local kyphotic deformity to sagittal imbalance of the whole spine. Furthermore, a local wedge shaped VP is a precursor for a new fracture due to the changes of the regional biomechanics.
Keeping these variates in mind should reduce the risk of adjacent fractures, but including this possibility on the informed consent makes a fracture of an adjacent VP an easier situation to handle.
Vertebroplasty versus Kyphoplasty
There are two claimed advantages of Balloon Kyphoplasty (BKP): less cement extravasation and better height restoration.
Cement extravasation
A meta-analysis showed that leakage of polymethyl metaacrylate (PMMA, standard cement) is present in 18.1% in BKP and 41.1% in VP. In VERTOS II, rates of up to 72% were reported. There seems to be no clinical relevance of a simple filling of a paravertebral vein (veinogram), but the extrusion to the disc space is a co-variate for adjacent level fractures. However, there are many more contributing factors, such as cement viscosity, special cannulas (side open with a controlled application to the desired direction), the surgeon’s experience, and desired total volume of cement filling.
Height restoration
The authors feel that a major reduction can only be achieved with the lordotic or relative lordotic positioning on the operating table, but there are many results in the literature reporting better restoration or maintaining height with additional inflation of the balloon and creation of a cavity.
Technical Aspects
Cement types
At the moment, there are not many alternatives to polymethyl metaacrylate (PMMA), which is the standard augmentation material. Calcium phosphate cements (CPC) and Calcium sulphate cements (CSC) exist but are not used on a large scale.
Amount of cement
Results from a national mandatory registry have shown that the higher cement volumes (3cc in the thoracic spine and 6cc in the lumbar spine) correlate with more pain relief.11 Other studies and clinical experience have demonstrated that in some cases minimal cement volume is enough for pain relieve.
Cost-Effectiveness
According to the model of quality-adjusted life years (QALY), cost-effectiveness was calculated by a Japanese group.18 Over an interval of 52 weeks, the gain of QALY has reached 0.162, EQ-5D (a general health score ) scores improved rapidly and continued to rise. Furthermore, the early application of vertebroplasty in acute fractures with a pain duration of less than six weeks lead to a significant reduction of hospital stay.8
SUMMARY
Vertebral body compression fractures due to osteoporosis are a tremendous burden on the aged and, because of the worldwide demographic shift to aging population, is an important socio-economic task to tackle. In patients with acute fractures (new collapse, history of pain less than six weeks with high pain levels) percutaneous minimally invasive transpedicular therapy options are of high benefit for patients.
REFERENCES
- United Nations. World Population Ageing [Report]. Department of Economic and Social Affairs Population Division. 2002; http://www.un.org/en/development/desa/population/publications/pdf/ageing/WPA2015_Report.pdf. Accessed March 9, 2019.
- Wade SW, Strader C, Fitzpatrick LA, Anthony MS. Sex- and age-specific incidence of non-traumatic fractures in selected industrialized countries. Arch Osteoporos. 2012;7:219-227.
- Aebi M Gunzburg R, Szpalski M (Eds). The Aging Spine. Berlin Heidelberg:Springer-Verlag;2005:viii, 131.
- Galibert P, Deramond H, Rosat P, Le Gars D. [Preliminary note on the treatment of vertebral angioma by percutaneous acrylic vertebroplasty]. Neurochirurgie. 1987;33(2):166-168.
- Buchbinder R, Osborne RH, Ebeling PR, et al. A randomized trial of vertebroplasty for painful osteoporotic vertebral fractures. N Engl J Med.2009;361:557-568. doi: 10.1056/NEJMoa0900429.
- Buchbinder R, Osborne RH, Kallmes D. Vertebroplasty appears no better than placebo for painful osteoporotic spinal fractures, and has potential to cause harm. Med J Aust. 2009;191(9):476-477.
- Klazen CA, Lohle PN, de Vries J, et al. Vertebroplasty versus conservative treatment in acute osteoporotic vertebral compression fractures (Vertos II): an open-label randomised trial. Lancet. 2010;376(9746):1085-1092.
- Clark W, Bird P, Gonski P, et al. Safety and efficacy of vertebroplasty for acute painful osteoporotic fractures (VAPOUR): a multicentre, randomised, double-blind, placebo-controlled trial. Lancet. 2016;388(10052):1408-1416.
- Wardlaw D, Cummings SR, Van Meirhaeghe J, et al. Efficacy and safety of balloon kyphoplasty compared with non-surgical care for vertebral compression fracture (FREE): a randomised controlled trial. Lancet. 2009;373(9668):1016-1024.
- Venmans A, Lohle PN, van Rooij WJ. Pain course in conservatively treated patients with back pain and a VCF on the spine radiograph (VERTOS III). Skeletal radiol. 2014;43(1):13-18.
- Roder C, Boszczyk B, Perler G, Aghayev E, Kulling F, Maestretti G. Cement volume is the most important modifiable predictor for pain relief in BKP: results from SWISSspine, a nationwide registry. Eur Spine J. 2013;22(10):2241-2248.
- Magerl F, Aebi M, Gertzbein SD, Harms J, Nazarian S. A comprehensive classification of thoracic and lumbar injuries. Eur Spine J. 1994;3(4):184-201.
- Abdelrahman H, Siam AE, Shawky A, Ezzati A, Boehm H. Infection after vertebroplasty or kyphoplasty. A series of nine cases and review of literature. Spine J. 2013;13(12):1809-1817.
- Pflugmacher R, Schroeder RJ, Klostermann CK. Incidence of adjacent vertebral fractures in patients treated with balloon kyphoplasty: two years' prospective follow-up. Acta Radiol. 2006;47(8):830-840.
- Yi X, Lu H, Tian F, et al. Recompression in new levels after percutaneous vertebroplasty and kyphoplasty compared with conservative treatment. Arch Ortho Trauma Surg. 2014;134(4):21-30.
- Movrin I. Adjacent level fracture after osteoporotic vertebral compression fracture: a nonrandomized prospective study comparing balloon kyphoplasty with conservative therapy. Wien Klin Wochenschr. 2012;124(9-10):304-311.
- Zhang H, Xu C, Zhang T, Gao Z, Zhang T. Does percutaneous vertebroplasty or balloon kyphoplasty for osteoporotic vertebral compression fractures increase the incidence of new vertebral fractures? A Meta-Analysis. Pain Physician. 2017;20(1):E13-E28
- Takura T, Yoshimatsu M, Sugimori H. Cost-effectiveness analysis of percutaneous vertebroplasty for osteoporotic compression fractures. Clin Spine Surg. 2017;30(3):E205-E210