
Kazuhiro Hasegawa and Kei Watanabe
INTRODUCTION
Posterior decompression surgery is the first choice of treatment for lumbar spinal stenosis (LSS) if conservative treatment fails. The goal of decompression is to relieve pressure on the nerve tissues while preserving the segmental stability. Because of the possible increase in the instability following a wide laminectomy,1-5 traditional decompression procedures for LSS have been improved and are still performed with limited resection of the facet joints.6 Since preservation of the facet joints and back muscles is the most important aspect to prevent postoperative segmental instability, the aim of minimally invasive lumbar decompression is to remove the ligamentum flavum without destroying the facet joints during decompression. Therefore, minimally invasive lumbar decompression for canal stenosis using a microscope7,8 or an endoscope9-11 is becoming a popular procedure for achieving this goal. Among the types of minimally invasive lumbar decompression surgeries, bilateral decompression through a unilateral approach using microendoscopic procedures,11,12 muscle-preserving interlaminar decompression (MILD)13 or microendscopic muscle-preserving interlaminar decompression (ME-MILD)14 are recently developed attractive procedures with decreased invasiveness not only to the facet joints but also to the back muscles, especially the multifidus muscle.
In this chapter, the authors clarify biomechanical difference in segmental instability following minimally invasive lumbar decompression compared with traditional procedures for LSS and destabilization models. We also present the anatomical detail of ligamentum flavum (LF), which plays a significant causative role in LSS. Based on the fundamental findings, we introduce a safe and reliable minimally invasive procedure with a video presentation.
Biomechanical Study on the Segmental Stability Following Minimally Invasive Decompression, Traditional Decompression, and Destabilization Procedures15
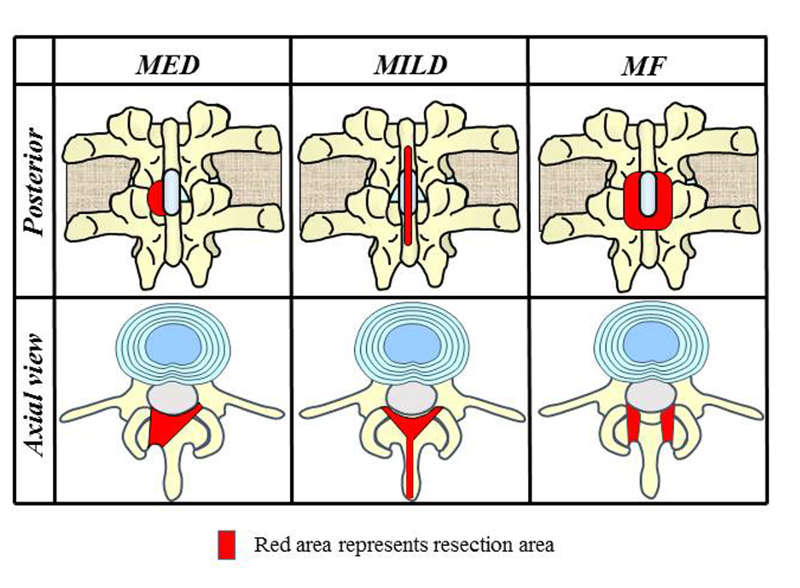
Thirty fresh frozen porcine functional spine units (FSUs) with preservation of the motion segment, including two vertebral bodies, the intervertebral disc, all ligamentous structures and back muscles were obtained from ten mature porcine lumbar spines of similar size and age (mean age 6 months; mean body weight 70 kg). The FSUs were mounted in a specially designed testing device16 that was connected to a stepper motor with a 6-axis load cell system via an analog-to-digital converter. Displacement of the steel box was measured using a Laser Displacement Sensor. The linear bushing, specimen, load cell and stepper motor were longitudinally connected for the torsional loading system. The mechanical tester was designed based on the universal spine tester reported in a previous article. All specimens were first tested intact in 3 axial motions on the mechanical testing machine: flexion-extension, right-left lateral bending and right-left axial rotation. Each motion was applied to the specimen from a neutral position up to 1.5° at a loading rate of 0.1°/second with application of a constant axial compression preload of 70 N.17 The specimens were then decompressed before retesting and were randomized to the following 5 decompression models: microendoscopic posterior decompression (MED), 9 muscle-preserving interlaminar decompression (MILD),13 bilateral medial facetectomy (MF),6 left unilateral total facetectomy and bilateral facetectomy (Fig. 5-1). The standardized stiffness and neutral zone (NZ), the most sensitive parameter,18 were calculated by dividing the value of the parameter obtained after the surgical procedures and destabilization procedures by the baseline value obtained in the intact specimen.
The mean standardized stiffness values of all loading modes tended to decrease in the order of MILD (0.984 N/mm), MED (0.942 N/mm), MF (0.833 N/mm), left unilateral total facetectomy (0.683 N/mm) and bilateral total facetectomy (0.433 N/mm). In contrast, the mean standardized neutral zone values tended to increase in the order of MILD (1.020 mm/N), MED (1.048 mm/N), MF (1.111 mm/N), left unilateral total facetectomy (1.787 mm/N) and bilateral total facetectomy (2.685 mm/N) (Fig. 5-2). Standardized NZ values in flexion following MED and MILD were lower than those following left unilateral total facetectomy and bilateral total facetectomy while there was no significant difference among MF, unilateral total facetectomy and bilateral total facetectomy. For the standardized NZ in extension, however, there was no significant difference between MED, MILD, MF and left unilateral total facetectomy. Standardized NZ in left torsion following MED, MILD and MF were equally lower to those of the destabilization models (Fig. 5-2).
FIGURE 5-2. Comparison of standardized neutral zone (NZ) among the surgical groups of microendoscopic decompression (MED),9 muscle-preserving interlaminar decompression (MILD),13 bilateral medical facetectomy (MF) ,6 left unilateral total facetectomy (UF) and bilateral total facetectomy (BF). The average values are shown in the graphs.
* p < 0.05 vs. BF
** p < 0.05 vs. UF & BF
Although overall results in the study show that even a conventional decompression procedure, MF, can maintain the segmental stability, MED or MILD, are preferable than MF when considering the result of flexion. Comparison of postoperative stability among MED, MILD and MF revealed that MILD tended to affect stability least, followed by MED and MF.
Anatomy of Ligamentum Flavum (LF) for Minimally Invasive Decompression Surgery19
Nerves are almost always compressed by the intervertebral disc and LF in LSS.20,21 Therefore total removal of ligamentum flavum (LF) is a basic procedure in the decompression surgery. On the other hand, intraoperative complication rate, especially dural injury during the procedure is still not negligible.22 Therefore, it is important to know the detail of anatomy of LF when surgical treatment is considered, because LF indicates the decompression area and also can play a role to protect the nerve tissues from injury due to drilling or resection of bony structure.
The authors investigated the anatomical details of LF using human cadaver (nine embalmed Japanese cadavers, seven males and two females, with a mean age of 74.2 years at the time of death, ages ranging between 59 and 96 years). At first, reconstruction-CT was taken for the en-bloc specimen after resection of all soft tissues from the spinal canal. Then, vertebral body was divided from the posterior elements at the pedicles and macroscopically observed whole aspect of LF. Then CT imaging with three-dimensional reconstruction was again performed for the posterior elements to clarify the location of LF. In the axial images of L4-L5 level, the cranial part, the disc level and the caudal part of LF attachments were investigated.
The whole shape of LF was like “a flying butterfly” toward cranial direction. There were distinct grooves of the nerve roots in the bone ceiling part of the foramen. LF attachment at the foraminal entrance was also clear. It was, however, difficult to distinguish the border between the capsular portion and the laminar portion macroscopically (Fig. 5-3). CT reconstructed images in the cranial section showed that although LF attachment at the midline is clear, the lateral part merges into the facet capsule (capsular portion). In the intervertebral disc level, LF covers the facet at the capsular portion. In caudal sections, LF attaches to the margin of the caudal lamina and the capsular portion is so thin that the laminar edge is close to the dural membrane (Fig. 5-3). These findings suggest that the margin of LF should be undercut at the cranial to the disc level, and the margin at the caudal portion be detouched while paying attention not to damage the nerve just beneath the thin LF.

Microendscopic Muscle-Preserving Interlaminar Decompression (ME-MILD)
Based on the aforementioned biomechanical and anatomical studies, we considered that ME-MILD is a desirable procedure for the decompression with total removal of ligamentum flavum preserving bilateral facet joint integrity and introduced ME-MILD as a routine procedure for LSS.14 The operation is carried out under general anesthesia with patients in a prone position on a Hall type frame. Following a 20-mm midline skin incision from the center of the crainial adjacent spinous process to the cranial edge of caudal adjacent spinous process, supraspinous ligament is longitudinally split at the median, and the dorsal surface of the spinous process is exposed. Preserving all the multifidus muscles, the spinous process is longitudinally split by a high-speed drill and fractured at the base of laminae, and the ligamentum flavum is exposed. Then, medical parts of inferior facets are also drilled. These procedures are done with a magnifying glass. A tubular retractor with a diameter of 16 mm is placed. Then, microendoscopic decompression using METRx microendoscopic discectomy system (Medtronic Sofamor Danek, Memphis, TN) is performed in the wide operative field. The caudal part of the upper vertebral lamina is resected sufficiently to reach the cranial edge of the ligamentum flavum, and the lateral recess is decompressed releasing the nerve root.
The patient is permitted to stand up and walk after recovery from anesthesia with a corset. A suction drainage tube is placed for 1 to 2 days to prevent postoperative epidural hematoma.
Case Presentation with Video
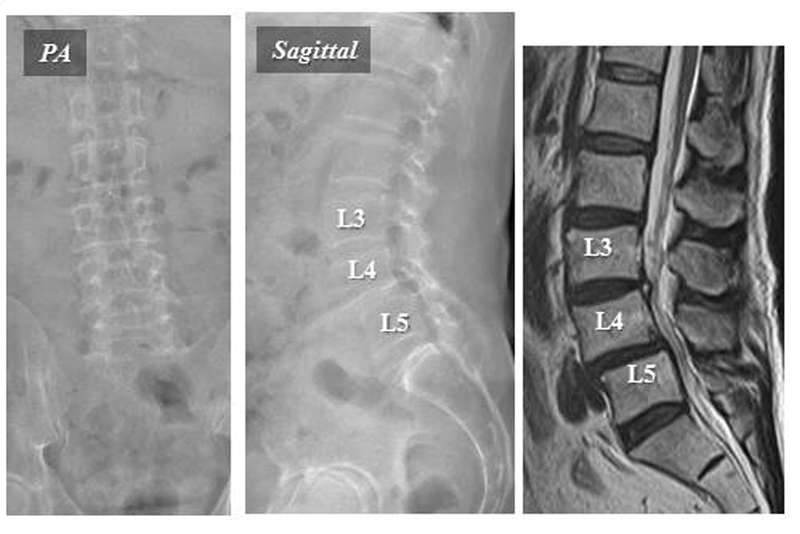
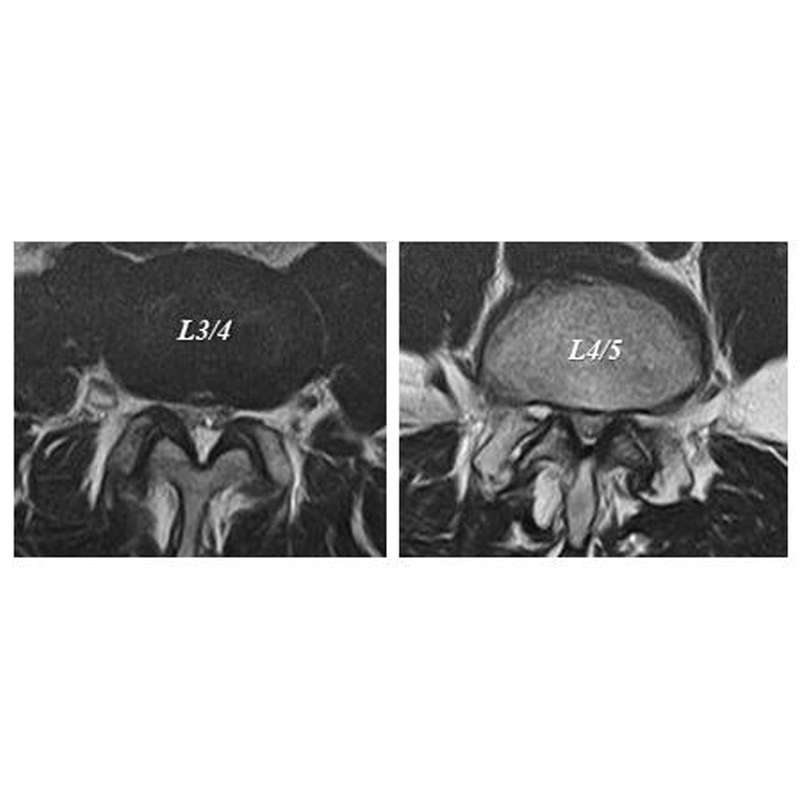
A 59-year-old man was referred by neurologic claudication. On presentation, he could not walk more than 100 m due to buttock to leg pain with Oswestry Disability Index (ODI) = 24.4%, Visual Analog Scale (VAS) (LBP/leg) = 35/80. Preoperative flexion-extension X-ray showed L4 degenerative spondylolisthesis (Fig. 5-4A). MRI demonstrated central type spinal canal stenosis at L3-4 and L4-5 without significant facet opening,23 indicating that the segments were stable (Fig.5-4B). Therefore, we scheduled ME-MILD for L3-4 and L4-5.
Following surgery, the symptoms were dramatically improved and he was enjoying normal daily activity with ODI =2.2% and VAS (LBP/leg) = 0/0 at postoperative one year. Radiographic evaluation demonstrated decompression of the spinal canal at L3-4 and L4-5 levels without deterioration of spondylolisthesis or facet joints (Fig. 5-4C).

CONCLUSION
The biomechanical study indicated that that muscle-preserving interlaminar decompression tended to affect stability least, followed by microendoscopic posterior decompression and bilateral medial facetectomy. Based on the biomechanical background, the authors initiate to perform decompression for LSS using microendscopic muscle-preserving interlaminar decompression (ME-MILD). The procedure realized safe removal of ligamentum flavum with least possible damage to the facet joints and back muscles. Therefore, ME-MILD is a promising option for a routine procedure of decompression surgery for LSS.
Video Presentation
Microendscopic Muscle-preserving Interlaminar Decompression (ME-MILD) Technique
REFERENCES
- Lee CK. Lumbar spinal instability (olisthesis) after extensive posterior spinal decompression. Spine (Phila Pa 1976). 1983;8:429-433.
- Johnsson KE, Willner S, Johnsson K. Postoperative instability after decompression for lumbar spinal stenosis. Spine (Phila Pa 1976). 1986;11:107-110.
- Hopp E, Tsou PM. Postdecompression lumbar instability. Clin Orthop Relat Res. 1988;227:143-151.
- Boden SD, Martin C, Rudolph R, Kirkpatrick JS, Moeini SM, Hutton WC. Increase of motion between lumbar vertebrae after excision of the capsule and cartilage of the facets. A cadaver study. J Bone Joint Surg Am. 1994;76(12):1847-1853.
- Bresnahan L, Ogden AT, Natarajan RN, Fessler RG. A biomechanical evaluation of graded posterior element removal for treatment of lumbar stenosis: comparison of a minimally invasive approach with two standard laminectomy techniques. Spine (Phila Pa 1976). 2009;34(1):17-23.
- Nakai O, Ookawa A, Yamaura I. Long-term roentgenographic and functional changes in patients who were treated with wide fenestration for central lumbar stenosis. J Bone Joint Surg Am. 1991;73(8):1184-1191.
- McCulloch JA, Young PH. Microsurgery for lumbar spinal canal stenosis. In: Essentials of Spinal Microsurgery. Philadelphia: Lippincott;1998:453-486.
- Weiner BK, Walker M, Brower RS, McCulloch JA. Microdecompression for lumbar spinal canal stenosis. Spine (Phila Pa 1976). 1999; 24(21):2268-2272.
- Foley KT, Smith MM. Microendoscopic discectomy. Tech Neurosurg. 1997;3:301-307.
- Khoo LT, Fessler RG. Microendoscopic decompressive laminotomy for the treatment of lumbar stenosis. Neurosurgery. 2002;51(5 Suppl):S146-S154.
- Yoshida M, Uwyoahi A, Maio K, Kawai M, Nakagawa Y. Surgical procedure and clinical results of endoscopic decompression for lumbar canal stenosis. In: Dezawa A, Chen PQ, Chung JY(eds). State of Art for Minimally Invasive Spine Surgery. Tokyo:Springer; 2005:15-24.
- Ikuta K, Arima J, Tanaka T, et al. Short-term results of microendoscopic posterior decompression for lumbar spinal stenosis. Technical note. J Neurosurg Spine.2005;2(5):624-633.
- Hatta Y, Shiraishi T, Sakamoto A, et al. Muscle-preserving interlaminar decompression for the lumbar spine: a minimally invasive new procedure for lumbar spinal canal stenosis. Spine (Phila Pa 1976). 2009;34(8):E276–E280.
- Mikami Y , Nagae M , Ikeda T, Tonomura H, Fujiwara H, Kubo T. Tubular surgery with the assistance of endoscopic surgery via midline approach for lumbar spinal canal stenosis: a technical note. Eur Spine J. 2013;22(9):2105-2112.
- Hasegawa K, Kitahara K, Shimoda H, Hara T. Biomechanical evaluation of destabilization following minimally invasive decompression for lumbar spinal canal stenosis. J Neurosurg Spine. 2013;18(5):504-510.
- Wilke HJ, Claes L, Schmitt H, Wolf S. A universal spine tester for in vitro experiments with muscle force simulation. Eur Spine J. 1994;3(2):91-97.
- Hasegawa K, Ikeda M, Washio T, Hara T. An experimental study of porcine lumbar segmental stiffness by the distraction-compression principle using a threaded interbody cage. J Spinal Disord. 2000;13(3):247-252.
- Panjabi MM, Goel VK, Takata K. Physiologic strains in the lumbar spinal ligaments. An in vitro biomechanical study. 1981 Volvo Award in Biomechanics. Spine (Phila Pa 1976). 1982;7(3):192-203.
- Yoshida M, Hasegawa K, Kageyama I, Maeda S, Kitahara K. An anatomical study of ligamentum flavum in reference to minimum invasive lumbar decompression. J Spine Res. 2015;6:103-109.
- Ramsey R. The anatomy of the ligamentum flavum. Clin Orthop Relat Res. 1966;44:129-140.
- Yong-Hing K, Reilly J, Kirkaldy-Willis W. The ligamentum flavum. Spine. 1976;1(4):226-234.
- Matsumoto M, Hasegawa T, Ito M, et al. Incidence of complication associated with spinal endoscopic surgery: nationwide survey in 2007 by Committee on spinal endoscopic surgery skill qualification of Japanese Orthopaedic Association. J Orthop Sci. 2010;15(1):92-96.
- Hasegawa K, Shimoda H, Kitahara K, Sasaki K, Homma T. What are the reliable radiological findings that indicate lumbar segmental instability? J Bone Joint Surg. 2011;93(5):650-657.