
Kazuhiro Hasegawa and Kei Watanabe
INTRODUCTION
Lumbar segmental instability is an unstable condition of the functional spinal unit of the lumbar spine. The definition is, however, yet to be clarified. In the clinical setting, evaluation of degenerative lumbar spines has been widely performed using X-ray measurement,1-7 but its usefulness for the diagnosis of segmental instability remains controversial because the large range of normal motion often overlaps underlying pathologic conditions.6,8 Furthermore, a conclusion about the biomechanical instability cannot be drawn from the functional X-rays, because the images do not provide information on load-deformation behavior. There are many outstanding ex-vivo and animal study reports on segmental instability;9-15 however, there is a gap between the experimental results and clinical instability. We have attempted to bridge the gap between the basic biomechanical data and the clinical manifestations induced by instability. Since 1997, we have developed a novel intraoperative measurement (IOM) system to investigate segmental biomechanical properties. This IOM system is the first clinically available method that can be used for measurement with all ligamentous structures intact and provides multiple parameters based on continuous load-deformation data (Fig.11-1).16 In this chapter, we will describe the basic concept, method, and clinical application of our IOM system.
MATERIALS AND METHODS
The IOM system incorporates spinous process holders (Gi-5, Mizuhoikakikai, Niigata, Japan), a motion generator (RC-RSW-L-50-S, IAI Corporation, Shimizu, Shizuoka), and a personal computer. The two holders are used to grip adjacent spinous processes firmly. A maximum cyclic displacement of 15.0 mm from the neutral position to both flexion and extension direction was generated at a speed of 2.0 mm/s to the tips of the holders. The neutral position was defined as that in which no load was recorded between the tips of the holders. Load at the tip of the caudal spinous process holders was measured with a load cell (LUR-A-200NSAI, Kyowadengyo Corporation, Chofu, Japan) and displacement was measured using an optical displacement transducer (LB-080, Keyence, Chofu, Japan). Real-time load-displacement data were recorded using a personal computer. The spinous process holder was connected to the motion generator through a multi-directional ball joint, producing flexion-extension of the segment (Fig. 11-1). The range of motion (ROM) induced by 15-mm craniocaudal displacements of the spinous processes was equivalent to approximately 9° of segmental flexion-extension.16
The patient is placed in the prone position on Hall's frame. The paraspinal muscles are detached from the spinous processes using standard procedures. Two spinous process holders are attached to the adjacent spinous processes. All ligamentous structures of the functional spinal unit, including the supra- and interspinous ligaments and facet joints, are kept intact. The motion generator attached to the tips of the holders loads the segment, producing five flexion-extension segmental motion cycles, and real-time load-displacement data are obtained with a sampling rate of 5 Hz. All the measurements using the IOM system were completed within 10 minutes without any complications related to the procedure. Data of the third cycle are used for biomechanical analysis. We obtained biomechanical parameters, stiffness and neutral zone (NZ),9 using the load-displacement data. Stiffness (N/mm) is defined as the slope of the line fitting the load-displacement curve from –15 mm to –10 mm on flexion. NZ (mm/N) is defined as the reciprocal of the load necessary to displace the two tips of the holders from a distance of -5 mm (flexion) to 5 mm (extension). All the lines used for measuring stiffness and NZ are calculated using the least-squares method (Fig. 11-1). In a previous series of 132 degenerative and eight normal segments that underwent measurement using the IOM system, we found that the NZs of all cases with normal discs were <2 mm/N. If NZ=2 is applied to the regression curve in the scattergram of stiffness and NZ: NZ=1.514-1.606*Log(Stiff), Stiffness=0.496, a lower value than the minimum Stiffness of normal segments.16 Therefore, instability was defined as a segment with NZ, the most reliable parameter for determining segmental instability,9 >2 mm/N (Fig. 11-2).
CLINICAL APPLICATIONS
Evaluation of Lumbar Degenerative Spondylolisthesis (LDS)17
LDS is considered a typical disease revealing lumbar segmental instability. Forty-eight patients with LDS (mean age: 68.5 years, men/women=19/29, Group D) who presented with neurogenic claudication were investigated by IOM system. Exclusion criteria of the subjects were a history of spinal surgery, spinal deformity, a metabolic disease affecting bone quality (e.g., osteoporosis), vascular disease of the lower extremities, and malignant disease. The age-matched control group included 48 lumbar spinal stenosis patients without spondylolisthesis (mean age: 64.8 years, men/women=33/15, Group N). None of the patients had a history of L5-S fusion or L5 sacralization. Symptoms and radiologic and biomechanical results were compared between the two groups. Symptoms were evaluated using the SF-36 (physical function) and visual analog scale utilizing the 100-mm method regarding low back and leg pain. Lateral X-rays with flexion-extension positions were obtained, and ROM was determined using Dupuis’ procedure.4 Standardized disc height (stDH) was calculated as the mean value of the anterior (DHa) and posterior disc height (DHp) divided by the anteroposterior width of the lower vertebra (W) as: stDH=(DHa+DHp)/W*100. A grade of spondylolisthesis was determined by the percentage of slippage (i.e., %slip). A grade of disc degeneration18,19 and Modic type20 were investigated by MRI (T2-weighted midsagittal fast spin-echo images).
Physical function of SF-36 (Group D: 50.4, Group N: 44.4), low back pain (visual analog scale; Group D: 63.5 mm, Group N: 65.3 mm) did not differ significantly between the groups. Leg pain was significantly greater in Group D (77.4) than in Group N (55.8). For the radiologic measurements, there was no significant difference between groups in the range of segmental motion, stDH, Thompson’s classification in magnetic resonance imaging (MRI), the frequency of Modic type 1 change, or computed tomography (CT) findings. The mean stiffness value (mean ± standard error) in Group D (0.686±0.03) had a tendency of lower value compared with Group N (0.797±0.04, p=0.0756), while the NZ in Group D (1.97±0.12) was significantly higher than that in Group N (1.73±0.14, p<0.05). The incidence of segmental instability (NZ>2mm/N), however, was not significantly different between groups. With a forward stepwise multivariate logistic regression on segmental instability, facet opening,21 subchondral sclerosis of the facet, type of facet joint,16 level of the disc for measurement (L3-4 vs. L4-5), stDH, and vacuum of the facet joint were selected as risk factors. Spondylolisthesis and ROM by X-ray evaluation were not predictors of instability. The logistic regression model following the stepwise regression analysis on segmental instability revealed that facet opening and facet type were significant factors, with an odds ratio >2 and p<0.05.
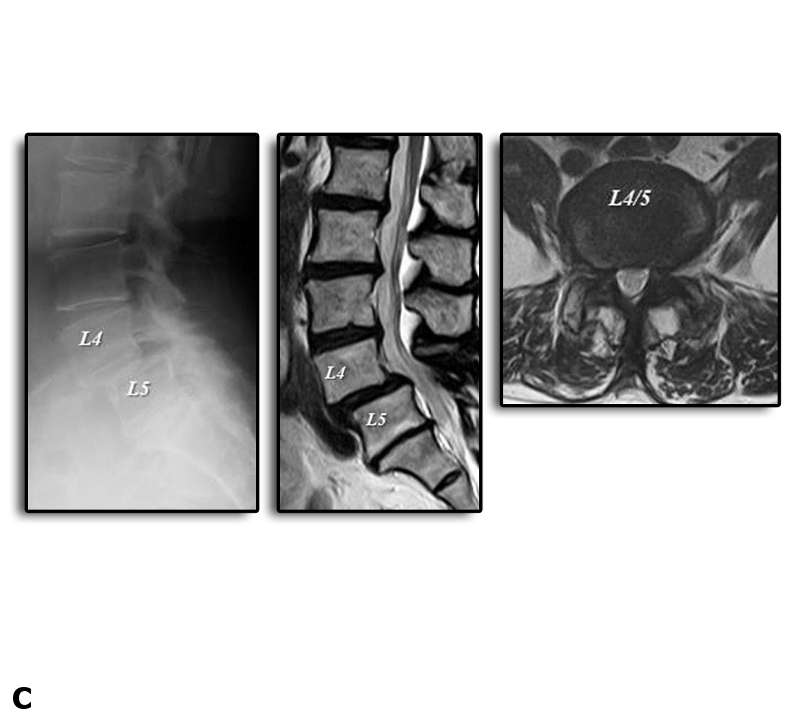
Our measurement system demonstrated that segments with spondylolisthesis (Group D) were characterized by lower flexion stiffness and a higher NZ compared to those without spondylolisthesis (Group N). However, neither the symptoms nor the frequency of instability differed significantly between groups. The results of this study demonstrated that LDS is not always unstable, suggesting that decompression alone is justified when the target segment is biomechanically stable (Figs. 11-3A, B, and C).
Relationship between Radiographic Findings and Biomechanical Characteristics Evaluated by IOM System16,21
We examined the reliability of radiological findings for lumbar segmental instability in patients with lumbar disease (n=112; mean age: 66.5 years, M/F=56/56) using IOM system. Risk factor analysis to predict instability was performed on X-ray (range of segmental motion, disc height), MRI (Thompson grade,18,19 Modic type,20 and axial CT findings of the facet (type, opening, vacuum, osteophyte, subchondral erosion, cyst, sclerosis) using a multivariate logistic regression with a forward stepwise procedure. Facet type was classified as sagittally oriented, coronally oriented, anisotropic, or wrapped. Stepwise multivariate regression analysis revealed that facet opening was the strongest predictor for instability, followed by spondylolisthesis, and MRI grade (Table 11-1). ROM by flexion-extension X-rays were not predictors of instability (Fig.11-4). NZ of the segment with normal disc was always <2.0 mm/N. On the other hand, NZ of the segment with degenerated disc, Grade 3 to 5, showed wide variation in the value with a tendency of higher NZ in degenerated disc, Grade 3 to 5, compared to NZ in normal discs, Grade 1 and 2 (Fig.11-5). Regarding clinical symptoms, SF-36 and VAS of the patients with instability were significantly more severe than those of the patient without instability. Furthermore, the surgical treatments determined using IOM system were effective, suggesting that segmental instability influences the symptoms of the lumbar degenerative diseases.
| Factor | Odd’s | p-value |
| Facet Opening | 5.6 | 0.014 |
| Spondylolisthesis | 2.8 | 0.058 |
| MRI:grade* | 2.6 | 0.145 |
Regarding facet opening, we investigated the relationship between facet joint volume determined by DICOM data from CT scans and biomechanical properties of the segment using IOM system in 29 patients17 with degenerative spondylolisthesis of the lumbar spine and 12 with spinal stenosis. The NZ was significantly greater in degenerative spondylolisthesis group than in spinal stenosis group (p<0.05) and significantly positively correlated with the average volume (R2=0.141, p<0.05), suggesting that an increased facet joint volume is an evidence of segmental instability in the degenerative lumbar spine.22
Case Presentation
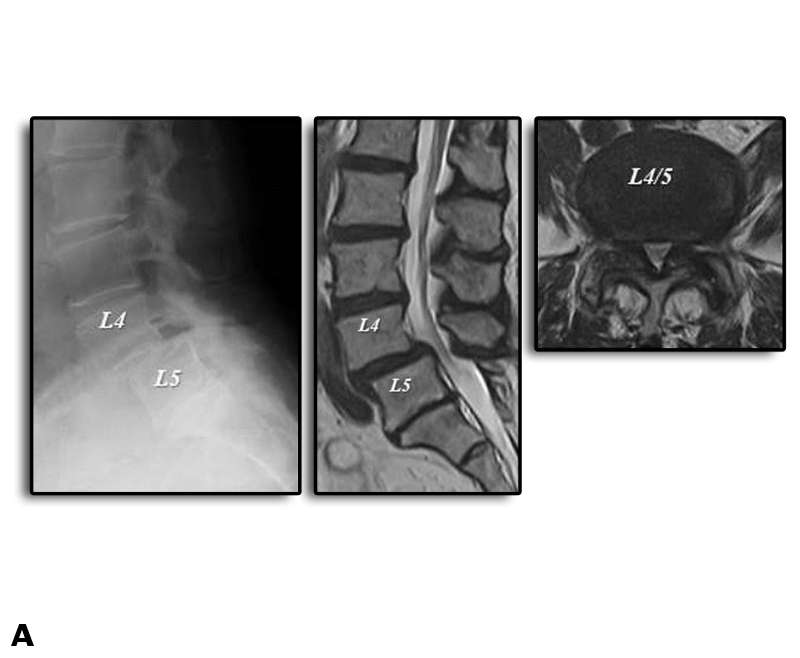
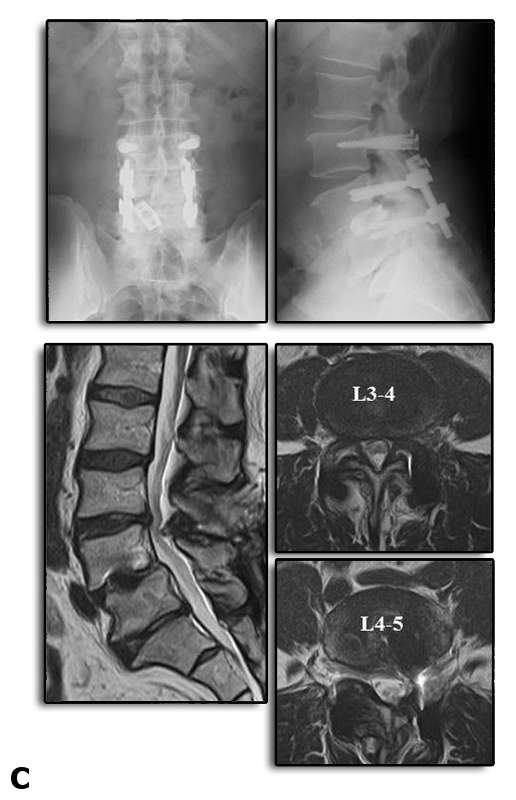
A 67-year-old man was referred by intractable mechanical low back pain and neurologic claudication. On presentation, he could not walk more than 50 m independently due to low back pain and bilateral leg numbness with SF-36(PF)=40, VAS (LBP/leg)=75/85. Preoperative flexion-extension X-ray showed degenerative spondylolisthesis (Fig. 11-6A). Central type spinal canal stenosis with segmental instability manifested by remarkable facet opening21,22 at L3-4 and L4-5 in T2-weighted MRI (Fig.11-6A).
Segmental motion evaluation at L3-4 and L4-5 with IOM system showed 0.4 N/mm in stiffness and 2.0 mm/N in NZ and 0.9 N/mm in stiffness and 2.6 mm/N in NZ, respectively (Fig. 11-6B). Based on the biomechanical result, we determined to perform TLIF for L4-5 and stabilization with pedicle screw based ligamentoplasty for L3-4. Following surgery, the symptoms were dramatically improved, and he was enjoying a normal daily activity with SF-36(PF)=95, VAS (LBP/leg)=20/10 two years after surgery. Radiographic evaluation revealed decompression of the spinal canal and stabilization of both segments. The facet opening had been resolved at L3-4 (Fig. 11-6C).

DISCUSSION
Intraoperative measurements of a cervical or lumbar segment are occasionally performed to determine instability.23-26 Common limitations of the previous devices include damage to the ligamentous or bone structures due to the fixation of pins, screws, or a spreader to the vertebrae, and also the fact that data about the stiffness of only a single loading direction, flexion, or extension are obtained. From a biomechanical viewpoint, it is clear that segmental properties of the spine cannot be determined by stiffness alone. Measurements of multiple parameters with at least NZ are necessary.9 The IOM system presented here is the first clinically available method that can be used for measurement with all ligamentous structures intact and provides multiple parameters based on continuous load-deformation data during surgery.16 There are, however, several limitations of the IOM system, for example, the measurement was performed in the segment after the paraspinal muscles were detached from the spinous process under general anesthesia in the prone position. Therefore, the condition of the measurement is not completely physiological, and the results represent the effects of passive stabilizers of the functional spinal unit.
CONCLUSION
Although there are several limitations in the method, we have achieved the following findings in the clinical trials using the IOM system, the first clinically available method that can be used for measurement with all ligamentous structures intact and provides multiple parameters based on continuous load-deformation data during surgery:
(1) Neutral zone, the sensitive parameter,9 was higher in the cases with mild disc degeneration and preserved disc height compared to the cases with a normal or severely degenerated disc, suggesting that degenerative segments with preserved disc height have a latent instability compared to segments with collapsed discs.16
(2) Comparison between the preoperative radiological findings and intraoperative measurements of the target segment with the IOM system in 112 patients with degenerative diseases demonstrated that facet opening, spondylolisthesis, and MRI grade (grades 3 and 4 versus grade 5) were risk factors.21 Regarding facet opening, the greater the facet joint volume the higher the neutral zone of the segment, suggesting that an increased facet joint volume, the facet opening, is an evidence of segmental instability in the degenerative lumbar spine.22
(3) The age-matched case-control study using the IOM system in forty-eight patients with degenerative spondylolisthesis and 48 lumbar spinal stenosis patients without degenerative spondylolisthesis about symptoms, radiologic, and biomechanical results revealed that degenerative spondylolisthesis is not always unstable, indicating that fusion surgery is not always indicated for patients with the pathology. 17
REFERENCES
- Knutsson F. The instability associated with disc degeneration in the lumbar spine. Acta Radiol. 1944;25:593-609.
- Morgan FP, King T. Primary instability of lumbar vertebrae as a cause of low back pain. J Bone Joint Surg Br. 1957;39-B(1):6-22.
- Pennal GF, Conn GS, McDonald G, Dale G, Garside H. Motion studies of the lumbar spine: a preliminary report. J Bone Joint Surg Br. 1972;54(3):442-452.
- Dupuis PR, Yong-hing K, Cassidy JD, Kirkaldy-Willis WH. Radiographic diagnosis of degenerative lumbar spinal instability. Spine (Phila Pa 1976). 1985;10(3):262-276.
- Frymoyer JW, Selby DK. Segmental instability. Rationale for treatment. Spine (Phila Pa 1976). 1985;10(3):280-286.
- Dvoák J, Panjabi MM, Chang DG, Theiler R, Grob D. Functional radiographic diagnosis of lumbar spine. Flexion-extension and lateral bending. Spine (Phila Pa 1976). 1991;16(5):562-571.
- Iguchi T, Kanemura A, Kasahara K, Kurihara A, Doita M, Yoshiya S. Age distribution of three radiologic factors for lumbar instability: probable aging process of the instability with disc degeneration. Spine (Phila Pa 1976). 2003;28(23):2628-2633.
- Hayes MA, Howard TC, Gruel CR, Kopta JA. Roentgenographic evaluation of lumbar spine flexion-extension in asymptomatic individuals. Spine (Phila Pa 1976). 1989;14(3):327-331.
- Panjabi MM, Goel VK, Takata K. Physiologic strains in the lumbar spinal ligaments. An in vitro biomechanical study 1981 Volvo Award in Biomechanics. Spine (Phila Pa 1976). 1982;7(3):192-203.
- Fujiwara A, Lim TH, An HS, et al. The effect of disc degeneration and facet joint osteoarthritis on the segmental flexibility of the lumbar spine. Spine (Phila Pa 1976). 2000;25(23):3036-3044.
- Gertzbein SD, Seligman J, Holtby R, et al. Centrode patterns and segmental instability in degenerative disc disease. Spine (Phila Pa 1976). 1985;10(3):257-261.
- Kaigle AM, Holm SH, Hansson TH. Experimental instability in the lumbar spine. Spine (Phila Pa 1976). 1995;20(4):421-430.
- Mimura M, Panjabi MM, Oxland TR, et al. Disc degeneration affects the multidirectional flexibility of the lumbar spine. Spine (Phila Pa 1976). 1994;19(12):1371-1380.
- Ogon M, Bender BR, Hooper DM, et al. A dynamic approach to spinal instability. Part I: Sensitization of intersegmental motion profiles to motion direction and load condition by instability. Spine (Phila Pa 1976). 1997;22(24):2841-2858.
- Panjabi MM, Krag M, Chung T. Effects of disc injury on mechanical behavior of the human spine. Spine (Phila Pa 1976). 1984;9(7):707-713.
- Hasegawa K, Kitahara K, Hara T, Takano K, Shimoda H, Homma T. Evaluation of lumbar segmental instability in degenerative diseases using a new intraoperative measurement system. J Neurosurg Spine. 2008;8(3):255-262.
- Hasegawa K, Kitahara K, Shimoda H, et al. Lumbar degenerative spondylolisthesis is not always unstable: clinicobiomechanical evidence. Spine (Phila Pa 1976). 2014;39(26):2127-2135.
- Thompson JP, Pearce RH, Schechter MT. Preliminary evaluation of a scheme for grading the gross morphology of the human intervertebral disc. Spine (Phila Pa 1976). 1990;15(5):411-415.
- Pfirrmann CW, Metzdorf A, Zanetti M, Hodler J, Boos N. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine (Phila Pa 1976). 2001;26(17):1873-1878.
- Modic MT, Steinberg PM, Ross JS, Masaryk TJ, Carter JR. Degenerative disk disease: assessment of changes in vertebral body marrow with MR imaging. Radiology. 1988;166(1 Pt 1):193-199.
- Hasegawa K, Shimoda H, Kitahara K, Sasaki K, Homma T. What are the reliable radiological findings that indicate lumbar segmental instability? J Bone Joint Surg Br. 2011;93(5):650-657.
- Hasegawa K, Kitahara K, Shimoda H, et al. Facet opening in lumbar degenerative diseases represents segmental instability. J Neurosurg Spine. 2010;12(6):687-693.
- Ebara S, Harada T, Hosono N, et al. Intraoperative measurement of lumbar spinal instability. Spine (Phila Pa 1976). 1992;17(3 Suppl): S44-50.
- Frank E, Chamberland D, Ragel B. A proposed technique for intraoperative measurement of cervical spine stiffness. Neurosurgery. 1996;39(1):147-150.
- Brown MD, Holms SH, Heiner AD, Wehman KF. Intraoperative measurement of lumbar spine motion segment stiffness. Spine (Phila Pa 1976). 2002;27(9): 954-958.
- Kanayama M, Hashimoto T, Shigenobu K, Oha F, Ishida T, Yamane S. Intraoperative biomechanical assessment of lumbar spinal instability: validation of radiographic parameters indicating anterior column support in lumbar spinal fusion. Spine (Phila Pa 1976). 2003;28(20):2368-2372.